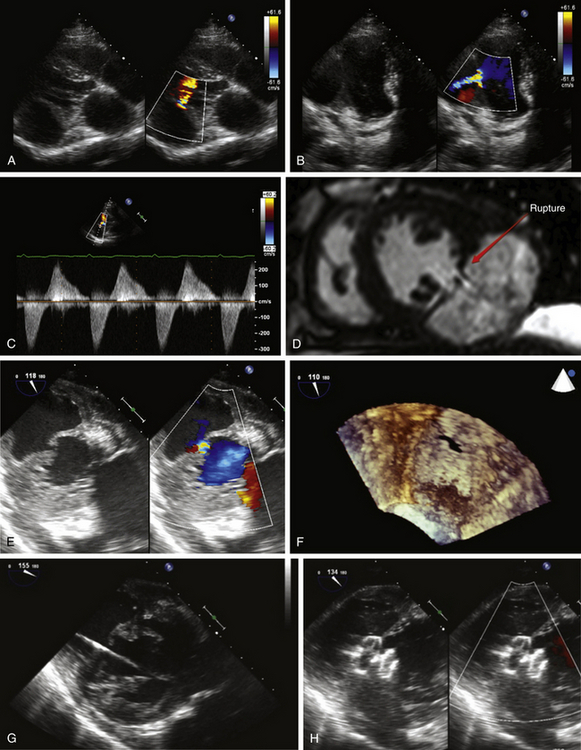
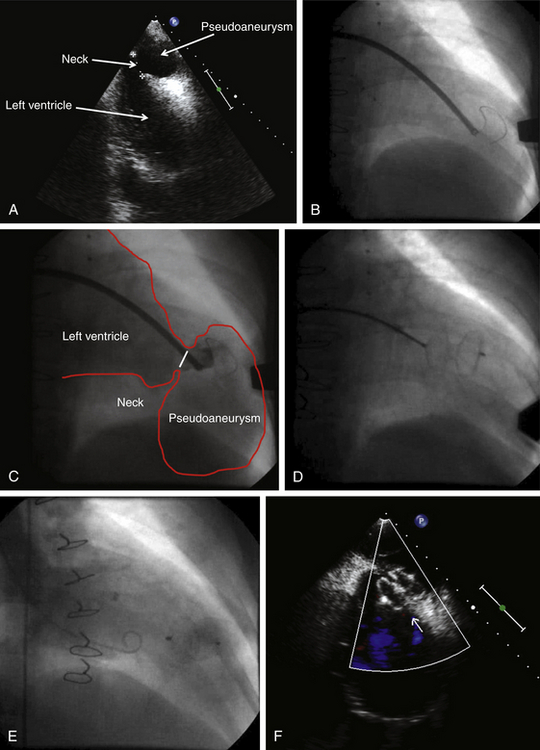
Chapter 18 There are three types of ventricular aneurysms: (1) true aneurysms that are outpouchings of ventricular segments (dyskinesis) involving the entire wall without disruption; (2) pseudoaneurysms that are disruptions of the entire ventricular free wall with blood extravasation into an extracardiac space with containment usually caused by overlying adhesive pericardium; and (3) pseudo-pseudoaneurysms (rare) that are partial disruptions of the ventricular wall, causing blood to enter and exit the ventricular wall.1–3 Pseudoaneurysms may be iatrogenic (previous thoracic surgery, most commonly mitral valve replacement), traumatic (e.g., stab wounds to the chest), secondary to infection (endocarditis), or in most cases, the consequence of myocardial infarction.4 Postinfarction rupture of the free wall usually results in pericardial hemorrhage and abrupt hemodynamic compromise and death,5 can be seen in 2% to 4% of myocardial infarctions, and is found in 23% of patients with fatal myocardial infarction at autopsy.6 Its occurrence seems to have a bimodal distribution with peaks early after the infarction (within 24 hours) and after 3 to 5 days. The incidence has decreased significantly in recent decades, likely the result of timely pharmacologic or mechanical reperfusion. In some cases, however, free wall rupture leads to a contained (by the fibrous adhesive parietal pericardium) extravasation of blood that may not be immediately apparent clinically and can be diagnosed years after the infarction. Although the main clinical concern is that pseudoaneurysms may rupture, there are no studies clarifying the natural history of pseudoaneurysms, particularly in patients in whom it is discovered years after the infarct. Additional concerns are heart failure related to ineffective delivery of blood into a noncontractile cavity, resulting in a compromise of forward cardiac output, and embolic events from thrombi located in the pseudoaneurysm cavity.7,8 The first challenge when faced with an outpouching of the left ventricular wall is the distinction between a pseudoaneurysm and true aneurysm. This can be difficult because on clinical grounds there are no features unique to either of the two entities that would allow confident distinction. Likewise, echocardiography will show dyskinetic myocardial motion in both cases and not uncommonly it is unclear whether the integrity of the myocardium is disrupted, particularly if thrombus is present within the cavity. It has been suggested that the ratio of the ostium of the cavity to the maximal cavity size may help in distinction between aneurysms and pseudoaneurysms with a ratio of less than 1:2 in favor of the latter and a ratio greater than 1:2 of the former. However, this criterion is less than perfect, and measurement of the ostium can be challenging echocardiographically. For example, in the largest analysis of pseudoaneurysms to date, the median ostium-to-pseudoaneurysm diameter ratio was 0.23, with a wide range (0.02 to 1.04), and less than 0.5 in only 75% of patients.4 Conventional coronary angiography together with left ventriculography may be helpful. Overlying coronary arteries are often seen in true aneurysms, whereas typically they are absent on the surface of a pseudoaneurysm.9 More recently, cardiac magnetic resonance imaging (MRI) has been reported useful,10–12 particularly in the distinction of thrombus from myocardium,12 and this should be part of the imaging work-up unless contraindicated or if other imaging modalities are diagnostic. It is also helpful in the assessment of the exact location, size, and characteristics of the ostium.10 Pseudoaneurysms are more commonly located posterior than anterior or apical.4 The natural history of pseudoaneurysms is unknown. Observational studies with limited numbers of patients suggest high mortality rates for untreated pseudoaneurysms.5,13,14 However, a selection bias does not allow definitive conclusions. For example, it is conceivable that patients with favorable clinical characteristics were selected for surgery, and those with prohibitive comorbidities associated with poor outcomes regardless of treatment were managed conservatively. The clinical presentation is variable, and some patients are incidentally found to have a pseudoaneurysm many years after the underlying myocardial infarction. In these patients the natural history may be much more favorable than in symptomatic patients with a pseudoaneurysm discovered shortly after the infarction. Traditionally, surgery has been considered the mainstay of therapy.15–17 In the largest series published to date, in 107 patients who underwent surgical pseudoaneurysm repair, follow-up study demonstrated that 23% of patients died at a median of 3 days after surgery.4 In 23 patients treated conservatively, the mortality was 48%. Deaths occurred early (median of 1 week after the infarct), and some patients were alive at 10 years’ follow-up study. At the writing of this chapter, there are no studies that compare outcomes after surgical and percutaneous repair, and data on percutaneous repair are limited to case reports.18–20 Suitability for percutaneous repair depends mainly on anatomical features. Most importantly, it must be determined whether the muscular rim surrounding the aneurysm neck is large enough to securely anchor a closure device. All closure devices are nitinol discs connected by a waist (ASD or VSD occluders such as Amplatzer septal occluders or ventricular septal occluders; St Jude Medical, St. Paul, Minn.); these are described more in detail in the respective chapters on ASD and VSD closure. Note that vascular plugs are typically not used because they do not offer the same stability for pseudoaneurysm closure as septal occluders or perimembranous VSD occluders—most vascular plugs do not have a sufficient waist. They are delivered via a guide catheter or sheath positioned into the pseudoaneurysm cavity. The minimum-access caliber depends on the anticipated device type and size and can be obtained by review of the manufacturer’s instructions for use. The waist diameter of the occluder should match or be slightly larger (1 to 2 mm) than the estimated diameter of the aneurysm neck, and the disc diameter should be at least 5 to 10 mm larger than the aneurysm neck. Attention to proper sizing allows secure anchoring without oversizing, which results in tension on surrounding structures including the pseudoaneurysm cavity or valvular apparatus. Femoral venous access is obtained, and after transseptal puncture, a soft-tipped, 0.035-inch, curved J-wire with a stiff or superstiff body is positioned into the pseudoaneurysm cavity. Alternatively, after femoral arterial access, a catheter is placed into the left ventricle and the wire positioned into the pseudoaneurysm cavity. Anticoagulation with intravenous heparin maintaining an anticoagulation time above 250 seconds is recommended. Subsequently, the guide catheter or delivery sheath is advanced over the wire into the pseudoaneurysm cavity. It is important never to be tempted to advance the guide catheter or sheath without a J-tipped wire positioned in the cavity to avoid injury of the containing aneurysm wall. Contrast injection into the pseudoaneurysm cavity will confirm appropriate sheath or catheter position and allow characterization of the aneurysm dimensions. Concomitantly, preferably three-dimensional transesophageal or intracardiac echocardiography should be considered to complement fluoroscopic imaging and to help with real-time device positioning. With the catheter or guide tip far enough in the pseudoaneurysm cavity, the wire is removed and the occluder is advanced to the distal sheath or catheter tip via a delivery cable. The sheath or catheter is slowly withdrawn while maintaining occluder position via the delivery cable until the distal occluder disc is desheathed. A gentle tug is applied to assure secure anchoring, and if confirmed, the sheath or catheter is withdrawn further, maintaining position of the delivery cable to allow the proximal disc to unfold. At this point contrast injection into the left ventricle is performed to assess device positioning, and adequate position is further confirmed via echocardiography. If the position is suboptimal, the occluder can be retrieved into the sheath and redeployed or a different occluder used. If the position is good, the occluder can be released by counterclockwise rotation of the delivery cable. Final cineangiography will confirm a successful occluder position. When an occluder is implanted into the inferior, posterior, or lateral wall, attention should be directed at the mitral apparatus and degree of mitral regurgitation before release because impingement on the mitral support structure can cause mitral regurgitation. In this case retrieval and repositioning or use of a different occluder type or size may be an alternative. It is important not to expect complete closure immediately because this may take weeks or months to occur. Complications include those related to access (e.g., subcutaneous, retroperitoneal, or rectus sheath hematomas; arteriovenous fistulae; pseudoaneurysms); embolic events secondary to insufficiently deaired guide catheters, sheaths, or devices, or to equipment-attached thrombi and thrombi originating from the pseudoaneurysm cavity; and cardiac perforations (e.g., of the aorta or left atrium during transseptal puncture or of the pseudoaneurysm cavity). The only possible treatment of a ruptured pseudoaneurysm cavity is emergency surgery with pericardiocentesis while preparing for emergency surgery. The risk of this complication depends on the age of the pseudoaneurysm and is more likely to occur with fresher pseudoaneurysms, the walls of which are more friable than those that have been present for many years. Figures 18–1 and 18–2 are examples of percutaneous repair of left ventricular pseudoaneurysms. Figure 18–1 This is the case of a 65-year-old male with prior coronary artery bypass surgery and coronary stenting on multiple previous occasions, as well as an inferior wall myocardial infarction treated with thrombolysis. The patient experienced chest pain and heart failure symptoms and was found to have a large left ventricular pseudoaneurysm with the entry point located in the posterior wall. Bypass grafts were patent on coronary angiography (not shown here). A and B demonstrate a parasternal long axis and an apical two-chamber view of the pseudoaneurysm respectively. The typical pattern of flow into and out of the aneurysm during systole and diastole is seen on Doppler interrogation in C. The pseudoaneurysm cavity is further assessed by cardiac magnetic resonance imaging (D) and transesophageal echocardiography (E), both of which are helpful in the assessment of the rim surrounding the neck as well as the neck diameter. F is the complementary three-dimensional en-face image of the pseudoaneurysm neck. In G, a superstiff 0.035-inch wire has been positioned into the pseudoaneurysm cavity, and in H, appropriate occluder position is confirmed with the muscular rim surrounding the pseudoaneurysm neck sandwiched between the two occluder discs. Figure 18–2 This is the case of a 42-year-old male who had undergone surgical left ventricular mass removal complicated by apical pseudoaneurysm formation that was subsequently closed with a Gore-Tex patch. Follow-up imaging demonstrated pseudoaneurysm enlargement and persistent extravasation of blood into the pseudoaneurysm cavity. A demonstrates a transesophageal echo view of the pseudoaneurysm, the left ventricle, and the neck. After venous access and transseptal puncture, a long sheath was placed into the left ventricular apex. B, A 0.035-inch J-tipped wire was positioned into the pseudoaneurysm cavity, and the sheath was advanced over the wire into the cavity. C, Contrast is injected into the pseudoaneurysm cavity. A 24-mm atrial septal defect occluder was released in a stepwise fashion with both discs sandwiching the rim of the aneurysm neck. D, A gentle tug is applied to the delivery cable to assure secure occlude position before release. E, The occluder is released and final left ventriculography performed with a pigtail catheter. F, Transesophageal echo demonstrates the occluder to be in a secure position.
Percutaneous Closure of Aortic, Coronary, and Ventricular Pseudoaneurysms and Coronary Fistulae
18.1 Left Ventricular Pseudoaneurysms
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Thoracic Key
Fastest Thoracic Insight Engine
