and Alessandra Cancellieri2
(1)
Department of Radiology, Bellaria Hospital, Bologna, Italy
(2)
Department of Pathology, Maggiore Hospital, Bologna, Italy
Radiology | Giorgia Dalpiaz | |
Pathology | Alessandra Cancellieri |
Nodular pattern | Definition | Page 98 |
|---|---|---|
Nodular signs | Low-density (subsolid) nodules High density (solid) nodules Cavitated nodules Calcified nodules Nodules with halo sign | Page 99 Page 100 Page 101 Page 101 Page 103 |
Subset lymphatic and table | Page 104 | |
Subset random and table | Page 105 | |
Subset centrilobular and table | Page 106 | |
Unusual distribution and table | Galaxy sign Cluster sign “Nodular” reversed halo sign | Page 108 Page 108 Page 109 |
Nodular Pattern
Definition
Nodular pattern is defined by the presence of multiple roundish pulmonary opacities ranging in diameter from 2 to 10 mm. Morphology, density, and distribution of the nodules depend on the route of arrival and the modality of spread.
Nodular pattern may be due to a variety of diseases arising directly in the lung or arriving via the bloodstream down to small vessels where they develop concentrically or via the bronchi.
The Nomenclature Committee of the Fleischner Society has recommended that the term “micronodule” be reserved for opacities less than 3 mm in diameter.
The signs of nodular pattern may be:
Low-density (subsolid) nodules
High-density (solid) nodules
Cavitated nodules
Calcified nodules
Nodules with halo sign
The prevalent distribution of the nodules together with the presence of non-parenchymal signs may be helpful for the diagnosis of a specific disease (please see the tables in this chapter).
As well as in nodular diseases, in which this pattern is predominant, there are other diseases in which nodules may be found, albeit less important or sporadic. They are therefore described in the corresponding chapters.
Boitsios G (2010) Diffuse pulmonary nodules. AJR Am J Roentgenol 194(5):W354
Chou SH (2013) Cheerio sign. J Thorac Imaging 28(1):W4
Gruden JF (1999) Multinodular disease: anatomic localization at thin-section CT – multireader evaluation of a simple algorithm. Radiology 210(3):711
Hansell DM (2008) Fleischner Society: glossary of terms for thoracic imaging. Radiology 246(3):697
Okada F (2007) Clinical/pathologic correlations in 553 patients with primary centrilobular findings on high-resolution CT scan of the thorax. Chest 132(6):1939
Pinto PS (2004) The CT halo sign. Radiology 230(1):109
Raoof S (2006) Pictorial essay: multinodular disease: a high-resolution CT scan diagnostic algorithm. Chest 129(3):805
Nodular Signs
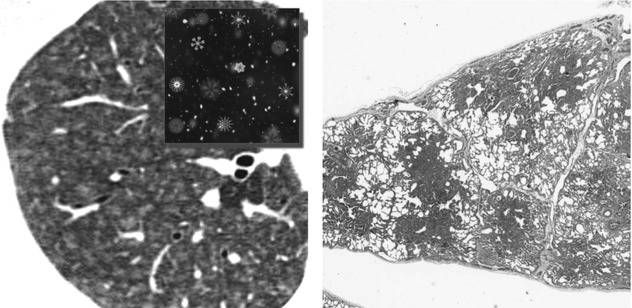
Low-density (subsolid) nodules
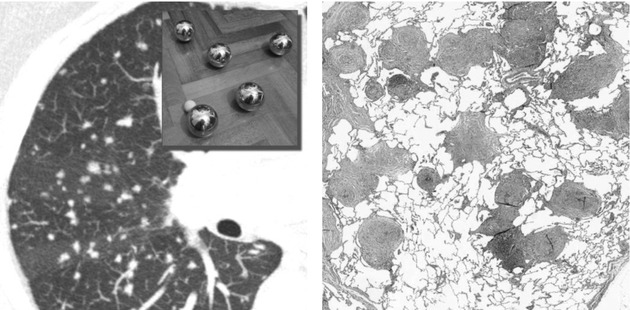
With a snowflake aspect (fluffy nodules), sometimes tiny and hence difficult to recognize, these low-density (subsolid) nodules may coalesce, resulting in the appearance of more or less extensive, patchy GGO. They are commonly seen in patients with diseases primarily affecting small airways and surrounding areas. The low-density CT aspect is due to minimal thickening of the peribronchiolar interstitium or partial filling of the peribronchiolar alveoli (e.g., subacute hypersensitivity pneumonitis; please see the pictures below). Both conditions are below the CT spatial resolution, and thus the common final effect is a focal low-density lesion. The ill-defined margins are due to a progressive reduction of interstitial or alveolar involvement extending away from the centrilobular area to the periphery.
Snowflake nodules, fluffy nodules, nodular GGO, ill-defined nodules, airspace nodules
Frequent diseases with low-density (subsolid) nodules:
Hypersensitivity pneumonitis (HP), subacute: it is the prototype disease of the snowflake nodules which are several and centrilobular (please see the figures above). The associated key sign for the diagnosis is the coexistence of sporadic lobular areas of air trapping appearing as patches of black lung. Another significant diagnostic finding, whenever present, is the so-called headcheese sign (please also refer to headcheese sign in chapters “Alveolar Pattern” and “Case-Based Glossary with Tips and Tricks”). Often the patient is a nonsmoker.
Respiratory bronchiolitis–interstitial lung disease (RB–ILD): in young heavy smokers, the presence of very tiny centrilobular snowflake nodules predominantly in the upper zones is suggestive for RB-ILD. These features are often in combination with areas of GGO and moderate centrilobular emphysema.
Rare diseases with Low-density (subsolid) nodules:
Follicular bronchiolitis (FB): in patients with collagen vascular disease (CVD), the presence of centrilobular tiny nodules associated with nodules mimicking a tree-in-bud pattern (peribronchiolar distribution) and cysts is suggestive for FB.
Hemorrhage (e.g., in endometriosis): the snowflake nodules are scattered and angiocentric, associated with patchy ground-glass opacities. Predictably, these lesions may vary in size during the menstrual cycle and may disappear after the cessation of menstruation.
Hot tub lung (HTL): the signs overlap with the reported findings of subacute HP. The key for the diagnosis is the possible coexistence of tiny, randomly distributed solid nodules with, of course, an anamnestic data of hot tub exposure.
Metastatic pulmonary calcification (MPC): in asymptomatic patients with hyperparathyroidism, the presence of centrilobular fluffy nodules (ground-glass nodular opacities) also containing foci of calcification mainly in the upper zones is suggestive for MPC. The frequently associated calcifications in the vessels of the chest wall support the diagnosis.
Pulmonary capillary hemangiomatosis (PCH): in young adults, the coexistence of widespread tiny snowflake nodules and lobular areas of ground-glass opacity with signs of pulmonary arterial hypertension is suggestive for PCH.
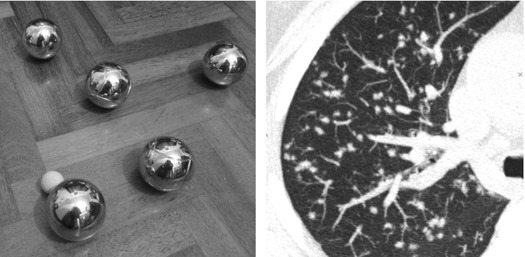
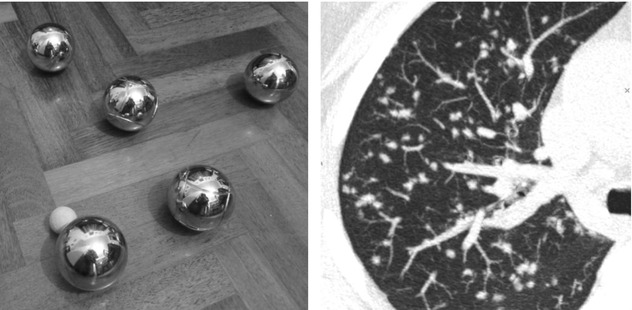
High Density (solid) Nodules
Being solid, these nodules obscure the edges of the vessels or other adjacent structures. Usually due to diseases primarily affecting the interstitium, they may coalesce in larger opacities or pseudoplaques. Regular or lobulated contours and even shaggy profiles are possible especially in diseases with a fibrotic component (e.g., sarcoidosis; please see the pictures below).
Interstitial nodules, ball-like nodules
Diseases with solid nodules:
Metastases, hematogenous: random solid nodules with well-defined margins and often prevalent at the bases and not uniform in diameter; crucial for the diagnosis are the other possible associated features of hematogenous diffusion such as pleural involvement and bone lesions, the latter often visible only with bone CT window.
Tuberculosis, miliary: numerous random tiny solid nodules, which are uniform in size; other associated findings which may possibly suggest the diagnosis include cavitation and signs of bronchogenic spread of the disease with tree-in-bud pattern; crucial also is the possible coexistence of hematogenous extrapulmonary involvement (please see the table in chapters “Alveolar Pattern” and “Alveolar Diseases” >Infection, chronic TB).
Sarcoidosis: lymphatic, with well-defined or shaggy margins and prevalent in the upper lobes (see the images above); crucial for the diagnosis is the coexistence of symmetrical hilar and mediastinal lymph nodes, also partially calcified.
Silicosis: lymphatic solid nodules often have well-defined margins, sometimes with calcifications; the nodules mainly involve the upper and posterior lung zones; crucial of course is the anamnesis of pneumoconiosis.
Lymphocytic interstitial pneumonia (LIP): the possible association of subpleural solid nodules with well-defined margins with sporadic cysts and ground-glass opacities is suggestive of LIP in patients with immunodeficiency syndromes and autoimmune disorders.
Langerhans cell histiocytosis (LCH), early: in smokers, the presence in the upper lobes of solid centrilobular, often cavitated, nodules, with possible shaggy margins and thick-walled cysts, is suggestive for LCH in florid phase.
Epithelioid hemangioendothelioma (EHE): multiple, usually bilateral, small solid nodules, mainly distributed in the subpleural space similar to metastatic lesions. EHE mainly affects young women and is usually asymptomatic.
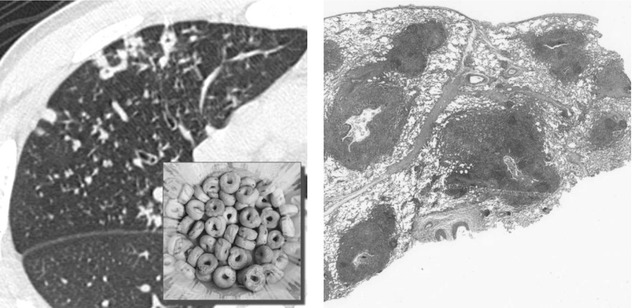
Cavitated Nodules
Cavitated nodules relate to pulmonary nodules with a central lucent cavity as seen on CT. It is due to the proliferation of (both neoplastic and nonneoplastic) cells around an airway or to necrosis (e.g., tuberculosis; please see the pictures below). They are named Cheerios after their resemblance to the breakfast cereals Cheerios.
Cheerio sign, Tarallucci sign (please also refer to the “Case-Based Glossary with Tips and Tricks”)