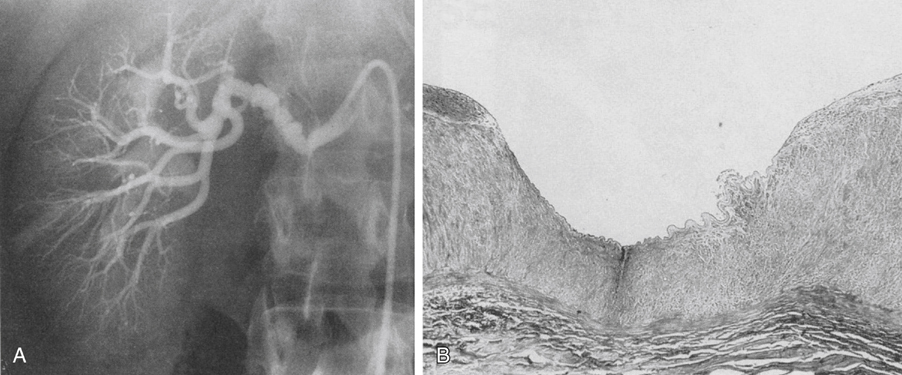
Primary intimal fibroplasia most often involves the main renal artery as a smooth focal stenosis (Figure lA). Segmental vessel intimal fibroplasia is uncommon but usually occurs as a weblike lesion. Irregularly arranged intimal mesenchymal cells surrounded by a loose matrix of connective tissue that produce circumferential narrowings of the vessel lumen typify primary intimal fibroplasia (Figure lB). The internal elastic lamina may be disrupted, but it is always present in these lesions. The cause of primary intimal fibroplasia is unknown. It is possible that this disease represents a proliferative remnant of fetal arterial musculoelastic cushions, similar to the intimal cushions that occur at cerebral artery bifurcations in adults. Lipid-containing foam cells and inflammatory cells are not present in this disease. Medial and adventitial tissues are usually normal in these vessels. Renal artery medial fibroplasia can occur as a solitary focal stenosis but is more common as a series of stenoses with intervening mural aneurysmal dilations. The thin-walled mural aneurysms have diameters exceeding that of the normal artery, and the stenoses appear as distinct webs projecting into the vessel lumen. Medial fibroplasia is most apt to affect the distal main renal artery (Figure 2A) and is bilateral in 55% of patients. In the presence of bilateral disease, the right-sided lesions usually appear more advanced. Unilateral disease affects the right side in 35% of patients and the left side in the remaining 10% of patients. These medial lesions extend into first-order segmental branches in approximately 25% of patients. The peripheral form of medial fibroplasia is characterized by the replacement of the smooth muscle of the outer media by compact fibrous connective tissue. Minimal accumulations of collagen and ground substances can affect the inner media of these vessels. Intimal tissues, the internal elastic lamina, and adventitial tissues are rarely affected. The diffuse form of medial fibroplasia is characterized by severe disorganization and loss of normal smooth muscle architecture, with excessive accumulations of fibrous tissue alternating with areas of marked medial thinning throughout the media (Figure 2B). Internal elastic lamina fragmentation and secondary intimal fibrosis may be present. Adventitial tissues usually appear normal in this form of renal artery disease.
Pathology of Arteriosclerotic, Fibrodysplastic, and Developmental Renal Artery Occlusive Disease
Renal Artery Fibrodysplasia
Intimal Fibroplasia

Medial Fibroplasia
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Thoracic Key
Fastest Thoracic Insight Engine
