Pathologic Processes Involving the Alveolar Spaces
Allen P. Burke, M.D.
Haresh Mani, M.D.
General
Alveolar pathology involves filling of alveolar spaces with acellular material (fluid, blood, protein, or matrix) or cells.
Edema
Transudates occur in the alveolar spaces generally in the absence of alveolar injury, but in the presence of venous hypertension (e.g., heart failure) and osmotic changes. The alveolar spaces are filled with lightstaining homogenous pink material, sometimes with tiny vacuoles, in the absence of fibrillar or granular structures (Fig. 3.1). Often, however, the edema fluid dissolves during tissue processing leaving emptyappearing alveolar spaces. Presence of dilated lymphatics and veins in interlobular septa and subpleural locations may then offer a clue to diagnosis, in the correct clinical setting.
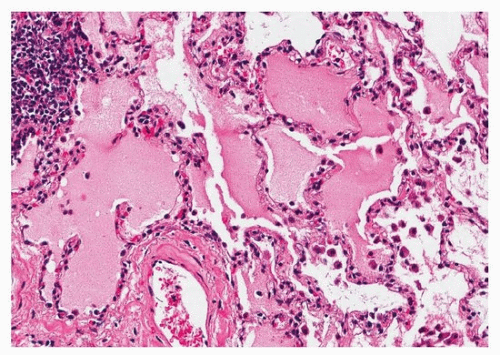 FIGURE 3.1 ▲ Pulmonary edema. There is a finely flocculent homogenous pink transudate filling the alveolar septa, with artifactual separation from the walls. There is no granularity or crystals to suggest proteinosis. Alveolar lining cells are nonreactive, and a fibrillary or ropy appearance to suggest fibrin is absent. |
Hemorrhage
As with fibrin, procedural hemorrhage is a common artifact. In order to suspect true hemorrhage, evidence of hemosiderin-laden macrophages (occurring in a few days, Fig. 3.2) or early phases of organization should be found. Pulmonary hemorrhage may be acute or chronic.
Surgical biopsies are rarely, if ever, performed to evaluate acute hemorrhage; more often, the pathologist may be asked to evaluate bronchoalveolar lavage (BAL) specimens in this setting. One must be cautious in interpreting iron stains on BAL specimens since so-called smoker’s macrophages also contain fine iron. Siderophages, on the other hand, contain coarse iron granules of varying sizes.
Surgical biopsies are rarely, if ever, performed to evaluate acute hemorrhage; more often, the pathologist may be asked to evaluate bronchoalveolar lavage (BAL) specimens in this setting. One must be cautious in interpreting iron stains on BAL specimens since so-called smoker’s macrophages also contain fine iron. Siderophages, on the other hand, contain coarse iron granules of varying sizes.
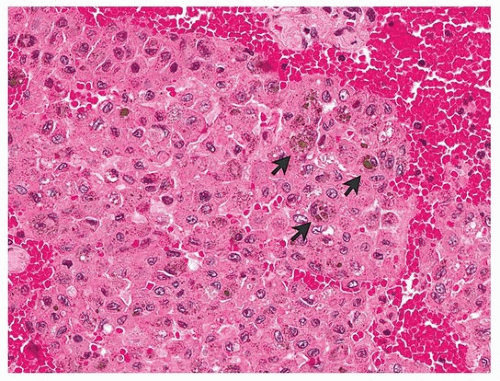 FIGURE 3.2 ▲ Pulmonary hemorrhage. In addition to intra-alveolar blood, there are scattered hemosiderin macrophages (arrows). Pulmonary alveolar lining cells are enlarged, and there are nonpigmented macrophages as well. |
 FIGURE 3.3 ▲ Intra-alveolar fibrin secondary to pneumonia. There is little acute inflammation, and the fibrin is fibrillar, with few red cells and dispersed inflammatory cells. |
The differential diagnosis of pulmonary hemorrhage is discussed in Chapter 32.
Fibrin
Fibrin is a common intra-alveolar process that should never be overlooked. Again, intact fibrin strands and red cells usually represent a procedural artifact. Early pathologic fibrin may maintain a fibrillar structure, but inflammatory cells are interspersed through it without layering or intact red cells (Figs. 3.3 and 3.4). Later, fibrin will show organization with endothelial cells at the periphery. A special form of fibrin mixed with necrotic alveolar lining cells results in hyaline membranes (Fig. 3.5; see Chapter 4). Fibrin may be focal and inconspicuous, usually accompanied by neutrophils, in areas of acute lung injury. The fibrin seen around pneumocystis pneumonia typically shows minute floccular clear spaces corresponding to the fungal organisms (Fig. 3.6). In general, any biopsy with acute lung injury should be stained for organisms (acid fast bacilli, gomori methenamine silver, tissue gram) and, if indicated, immunohistochemical stains for viruses. In practice, presence of prominent alveolar fibrin should raise a differential diagnosis of diffuse alveolar damage, acute fibrinous and organizing pneumonia, and pulmonary hemorrhage syndromes.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


