Pancoast’s Tumor
Presentation
A 59-year-old man is referred to your office with right shoulder pain. Past medical history is significant for dyspnea on moderate exertion (two flights of stairs) and pneumonia 5 years previously that required hospitalization. The patient reports no history of trauma but a 40-pack-per-year smoking history. He has worked at a desk job his entire life and has not had any recent travel abroad.
▪ Chest X-rays
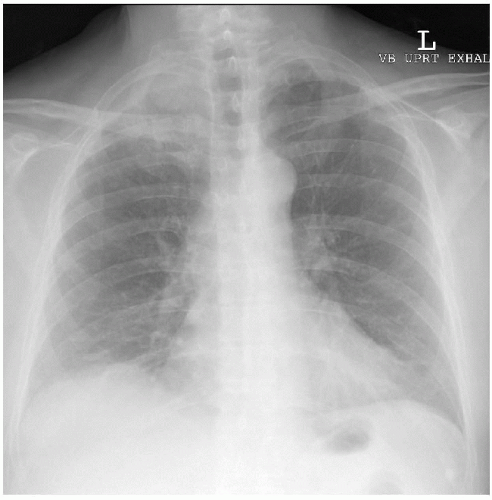 Figure 55-1 |
 Figure 55-2 |
Chest X-ray Report
Chest x-rays demonstrate a large lobulated mass involving the right lung apex with apparent destruction of the medial aspect of the third rib on the right side. There is left apical pleural thickening. There are no other parenchymal abnormalities, and the hilum and mediastinum are normal in appearance. This lesion is commonly referred to as Pancoast’s tumor.
Case Continued
The finding of rib destruction on chest x-ray most often implies a malignant etiology as opposed to an infectious process. History of smoking with an associated lung mass suggests a lung primary as opposed to a primary bone tumor with extension into the lung. Chest computed tomography (CT) scans, which include the liver and the adrenal glands, help to delineate the abnormality in the right lung apex. In addition, CT scans help to assess the right hilum, mediastinum, liver, and adrenals.
▪ CT Scans
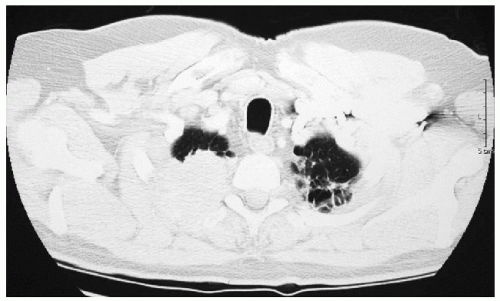 Figure 55-3 |
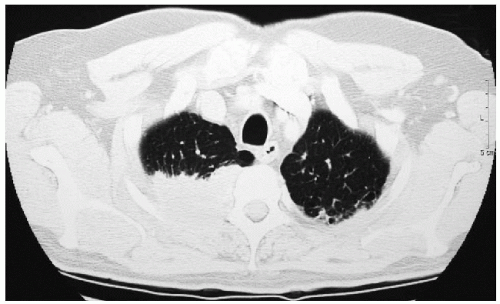 Figure 55-4 |
CT Scan Report
The CT scans demonstrate a posteriorly based 6-cm × 5-cm mass in the right lung apex associated with destruction of the posterior portion of the right third rib. There is scarring at the left lung apex posteriorly but no other parenchymal abnormalities within either lung. There is no evidence of hilar or mediastinal lymphadenopathy (all lymph nodes smaller than 1 cm in short-axis diameter). The liver and adrenal glands are normal.
Discussion
Tumors of the lung apices can invade the chest wall early in the course of the disease because of the close proximity of the apex of the lung to the chest wall. Patients are symptomatic more often when tumors are located in this area. Invasion of the stellate ganglion is common and results in a Horner’s syndrome. Shoulder and arm pain radiating down the C8 to T1 distribution are also common. Pathologic confirmation of the suspected tumor is required because a small number of patients may have small cell carcinoma, which necessitates a different treatment regimen. Bronchoscopy with transbronchial biopsy under fluoroscopic guidance yields a diagnosis in only 10% to 30% of patients. A CT-guided lung biopsy has a high yield in establishing a diagnosis with a low risk for a pneumothorax because the tumor is adherent to the chest wall.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


