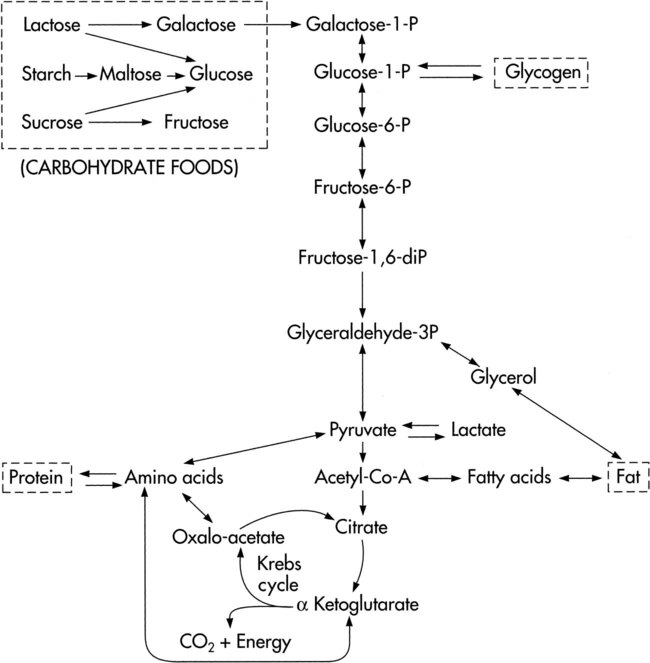
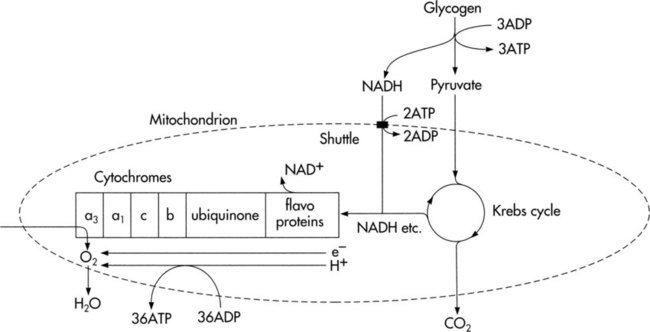
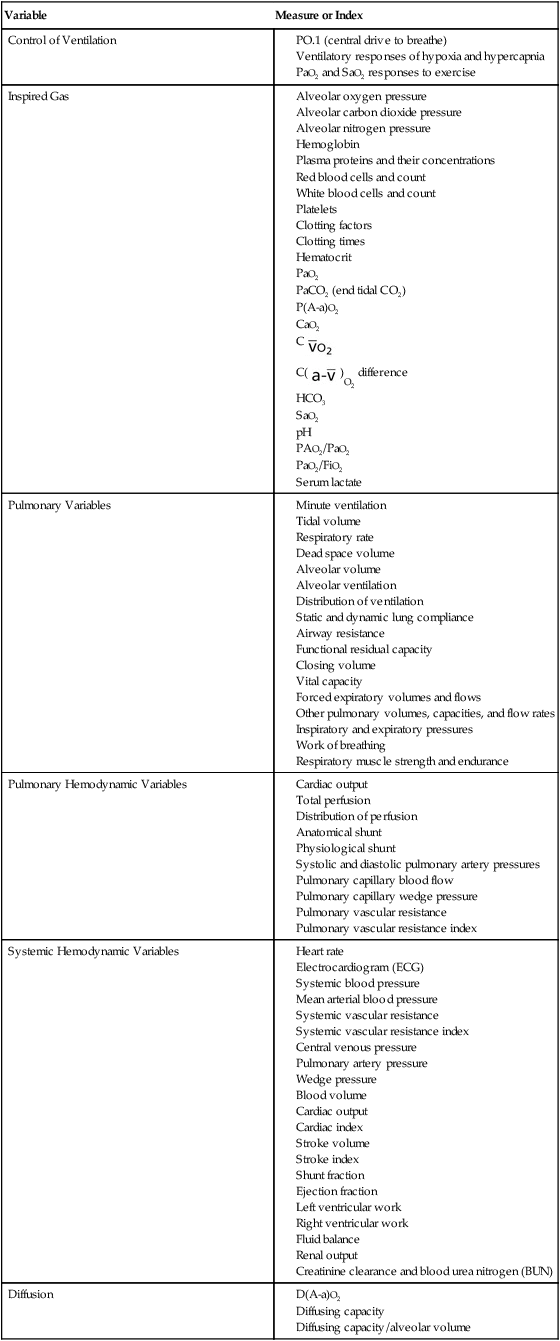
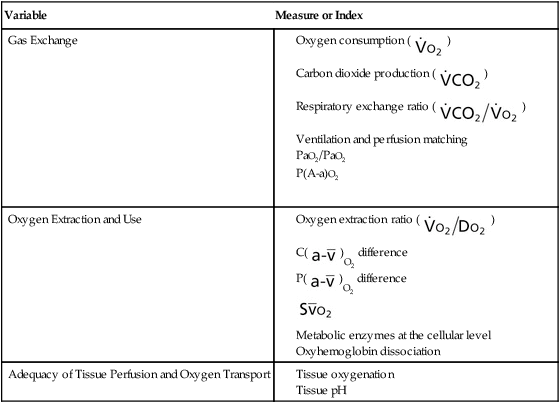
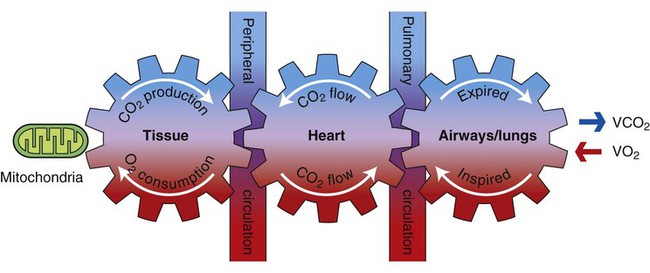
Oxygen transport is essential to life, activity, and participation in life consistent with the International Classification of Functioning, Disability and Health (ICF).1 Maximizing the efficiency of the oxygen transport pathway promotes optimal mobility and independence, the cornerstones of quality of life and well-being. Attention to oxygen transport—its deficits and threats to it—is the concern of physical therapists, irrespective of the primary clinical area of their practices. This is particularly true given the trend toward physical therapists’ direct access to patients and the prevalence of lifestyle-related conditions, all of which affect oxygen transport either directly or indirectly. Oxygen transport refers to the delivery of fully oxygenated blood to peripheral tissues, cellular uptake of oxygen, use of oxygen within the tissue, and the return of partially desaturated blood to the lungs. The oxygen transport pathway consists of multiple steps ranging from the ambient air to the perfusion of peripheral tissues with oxygenated arterial blood (Figure 2-1). Oxygen transport has become the basis for conceptualizing cardiovascular and pulmonary function and diagnosing and managing cardiovascular and pulmonary dysfunction.2–8 Oxygen transport variables include oxygen delivery (DO2), oxygen consumption ( Measures and indexes of oxygen transport that reflect the function of the component steps of the oxygen transport pathway are shown in Table 2-1. Table 2-1 Measures and Indexes of the Function of the Steps in the Oxygen Transport Pathway Cellular metabolism and survival depend on the continuous synthesis and degradation of adenosine triphosphate (ATP), the major source of energy for biological work. Work is performed in biological systems for contraction of skeletal, cardiac, and smooth muscle (e.g., exercise, digestion, glandular secretion, and thermoregulation) and for nerve impulse transmission (Box 2-1). These processes require a continuous supply of ATP, which is made available primarily by aerobic (oxygen-requiring) processes. In the event that oxygen delivery is inadequate, nonaerobic (anaerobic, or non–oxygen-requiring) energy-transferring processes can also supply ATP. Supplying energy anaerobically, however, is more costly metabolically; that is, it is not efficient, is limited, and cannot be sustained because of the disruptive effects of lactate (a cellular byproduct of anaerobic metabolism) on physiological processes. Metabolic acidosis is a consequence of lactate accumulation. In patients who are critically ill, the presence of metabolic acidosis secondary to anaerobic metabolism can be life threatening. Prolonged anaerobic metabolism is lethal in two respects. First, the patient is increasingly dependent on anaerobic metabolism because of inadequate DO2 to peripheral tissues; second, acidosis interferes with normal cellular processes and homeostasis, which require an optimal pH of 7.40. The complex, enzymatically controlled chemical reactions of metabolism are designed to form and conserve energy through the Krebs cycle and the electron transfer chain and then use this energy for biological work.9,10 Carbohydrates, fats, and proteins ingested from foodstuffs in the diet are oxidized to provide the energy for phosphorylation of adenosine diphosphate (ADP) (i.e., the formation of ATP by combining ADP with phosphate). These substances are broken down, and they access the Krebs cycle at the pyruvic acid or acetyl coenzyme A (CoA) levels (Fig. 2-3). Some amino acids can enter the Krebs cycle directly. Cellular oxidation, or respiration, refers to the function of the electron transfer chain to release energy in small amounts and to conserve energy in the formation of high-energy bonds. It is this process that ensures a continual energy supply to meet the needs of metabolism (Fig. 2-4). Three major systems of energy transfer exist to supply energy during all-out exercise over varying durations.10 Although these systems are discrete, they overlap. Cellular ATP and creatine phosphate (CP) are immediate energy sources for the first 10 seconds of exercise. From 30 to 60 seconds, glycolysis provides a short-term energy source. The ATP-CP system and the glycolytic system are anaerobic processes. As exercise persists for several minutes, the long-term aerobic system predominates. Thus, for sustained physical activity and exercise, energy is provided primarily by aerobic metabolism. For this process, oxygen is provided by the oxygen transport pathway. Carbon compounds that enter the body in the form of carbohydrate, fat, and protein undergo oxidative metabolism in the form of aerobic glycolysis in the mitochondria in the cytoplasm of cells. The basic mechanism for muscle contraction is excitation contraction coupling.11,12 Action potentials mediated centrally or through the spinal cord depolarize the muscle cell membrane (the sarcolemma) and stimulate the release of calcium from the lateral sacs of the sarcoplasmic reticulum. The sarcoplasmic reticulum is an extensive network of invaginations and tubular channels encasing the muscle fibers (myofibrils). The calcium floods over the myofilaments of the myofibrils within the sarcomere. Myofilaments consist of thin actin fiber and thick myosin fiber protein, which interdigitate with each other, giving the typical striated appearance to skeletal muscle (Fig. 2-5
Oxygen Transport
The Basis of Cardiovascular and Pulmonary Physical Therapy
Oxygen Transport
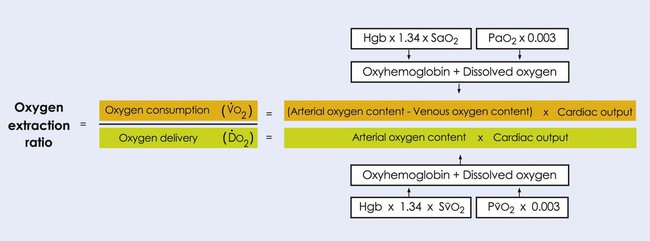
 ), and the oxygen extraction ratio (OER), the utilization coefficient. Oxygen demand is the amount of oxygen required by the cells for aerobic metabolism. Oxygen demand is usually reflected by
), and the oxygen extraction ratio (OER), the utilization coefficient. Oxygen demand is the amount of oxygen required by the cells for aerobic metabolism. Oxygen demand is usually reflected by  ; however, in cases of severe cardiovascular and pulmonary dysfunction and compromise to oxygen transport,
; however, in cases of severe cardiovascular and pulmonary dysfunction and compromise to oxygen transport,  can fall short of the demand for oxygen. Oxygen transport variables, including the components of DO2,
can fall short of the demand for oxygen. Oxygen transport variables, including the components of DO2,  , and OER, are shown in Figure 2-2. DO2 is determined by arterial oxygen content and cardiac output,
, and OER, are shown in Figure 2-2. DO2 is determined by arterial oxygen content and cardiac output,  by the arteriovenous oxygen content difference and cardiac output, and oxygen extraction by the ratio of DO2 to
by the arteriovenous oxygen content difference and cardiac output, and oxygen extraction by the ratio of DO2 to  .
.
Variable
Measure or Index
Control of Ventilation
Inspired Gas
Pulmonary Variables
Pulmonary Hemodynamic Variables
Systemic Hemodynamic Variables
Diffusion
Gas Exchange
Oxygen Extraction and Use
Adequacy of Tissue Perfusion and Oxygen Transport
Energy Transfer and Cellular Oxidation
Muscle Contraction and Metabolism
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Oxygen Transport: The Basis of Cardiovascular and Pulmonary Physical Therapy
 ), and oxygen extraction ratio (OER).
), and oxygen extraction ratio (OER). 
 )
) )
) )
) )
) )
) )
) )
)