Although high-degree atrioventricular block (AVB) is a common initial manifestation of cardiac sarcoidosis, little is known about the outcomes. The aim of this study was to assess outcomes in patients with AVB as an initial manifestation of cardiac sarcoidosis compared with those in patients with ventricular tachyarrhythmia (VT) and/or heart failure (HF). Fifty-three consecutive patients with cardiac sarcoidosis, who had high-degree AVB (n = 22) or VT and/or HF (n = 31), were enrolled. The end point was defined as major adverse cardiac events, including cardiac death, ventricular fibrillation, sustained VT, and hospitalization for HF. Over a median follow-up period of 34 months, the outcomes of major adverse cardiac events were better in patients with high-degree AVB than in those with VT and/or HF (log-rank test, p = 0.046). However, this difference was due mainly to HF hospitalization. The outcomes of fatal cardiac events, including cardiac death, ventricular fibrillation, and sustained VT, were comparable between the 2 groups (log-rank test, p = 0.877). The fatal cardiac events in patients with high-degree AVB were not associated with the initiation of steroid treatment or left ventricular dysfunction. In conclusion, the outcomes of major adverse cardiac events are better in patients with high-degree AVB than in those with VT and/or HF. However, patients with high-degree AVB have a high rate of fatal cardiac events, similar to those with VT and/or HF. An indication for an implantable cardioverter-defibrillator, but not a pacemaker system, can be considered in patients with cardiac sarcoidosis manifested by high-degree AVB.
Sarcoidosis is a systemic granulomatous disease of unknown origin. Cardiac involvement is increasingly recognized because of adverse outcomes. The principal initial manifestation of cardiac sarcoidosis is high-degree atrioventricular block (AVB), ventricular tachyarrhythmia (VT), or heart failure (HF). Patients with VT have a high rate of recurrence of fatal VT or sudden cardiac death. HF caused by left ventricular dysfunction is one of the most common causes of cardiac death. Therefore, patients with VT and/or HF as the initial manifestation of cardiac sarcoidosis are regarded as at high risk for cardiac events, whereas outcomes in patients with high-degree AVB have not been well investigated. One study showed that patients with AVB caused by cardiac sarcoidosis had an increase in the risk for cardiac events compared with those with idiopathic AVB. However, whether the outcomes are different according to the initial manifestation, such as high-degree AVB or VT and/or HF, remains unknown. Understanding the incidence of cardiac events in patients with high-degree AVB may be important for selecting the appropriate device (i.e., pacemaker system vs implantable cardioverter-defibrillator [ICD]). The aim of this study was to assess outcomes in patients with high-degree AVB as the initial manifestation of cardiac sarcoidosis compared with those in patients with VT and/or HF.
Methods
The study population consisted of 53 consecutive patients diagnosed with cardiac sarcoidosis in our institution from July 1998 to November 2013, who had high-degree AVB (n = 22) or VT and/or HF (n = 31) as the initial manifestation. Cardiac sarcoidosis was diagnosed according to Japanese Ministry of Health and Welfare guidelines, revised in 2006 by the Japanese Society of Sarcoidosis and Other Granulomatous Disorders. In brief, cardiac sarcoidosis is diagnosed on the basis of histologic findings or clinical findings. Histologic diagnosis is confirmed when endomyocardial biopsy specimens demonstrate noncaseating epithelioid cell granulomas. Clinical diagnosis is confirmed in the absence of endomyocardial biopsy when extracardiac sarcoidosis is diagnosed and the following clinical cardiac criteria (>2 of 4 major criteria, or 1 of 4 major criteria and >2 of 5 minor criteria) is satisfied. Major criteria consist of advanced AVB, basal thinning of the interventricular septum, positive myocardial uptake of gallium-67 citrate ( 67 Ga) scintigraphy or 18 F-fluoro-2-deoxyglucose ( 18 F-FDG) positron emission tomography (PET), and a left ventricular ejection fraction <50%. Minor criteria consist of abnormal electrocardiographic results, abnormal echocardiographic results, perfusion defect on thallium-201 or technetium-99m myocardial scintigraphy, delay enhancement of myocardium on gadolinium-enhanced cardiac magnetic resonance imaging, and interstitial fibrosis or monocyte infiltration on endomyocardial biopsy. This study was performed according to the principles of the Declaration of Helsinki and was approved by the institutional ethics committee.
This was a retrospective observational study. Patients with high-degree AVB were defined as having complete AVB or Mobitz II block at the time of initial manifestation of cardiac sarcoidosis. Patients with VT and/or HF were defined as having ventricular fibrillation or sustained VT and/or as being hospitalized for HF caused by left ventricular dysfunction without high-degree AVB, at the time of initial manifestation. Sustained VT was defined as spontaneous ventricular tachycardia at a rate of ≥120 beats/min that lasted ≥30 seconds. Steroid treatment was initiated at a dose of 30 or 40 mg/day of prednisone. Doses of prednisone were tapered over a period of 6 to 12 months to maintenance doses of 5 to 10 mg daily.
The end point was defined as major adverse cardiac events, including cardiac death, ventricular fibrillation, sustained VT, and hospitalization for HF. Patients were followed from the date of initial manifestation of cardiac sarcoidosis, such as high-degree AVB or VT and/or HF hospitalization, until the date of first documentation of cardiac events or the end of follow-up, whichever occurred first. The first documentation of cardiac events was assessed after the initial manifestation had been recovered. Follow-up information was obtained by medical records, contact with the patient’s physicians, or telephone interview with the patient or, if deceased, with family members.
Gallium-67 citrate scintigraphy was performed in all patients. Fluorine-18-FDG PET was performed in 6 patients who were diagnosed after September 2010 and had no positive myocardial uptake of 67 Ga at baseline. On 18 F-FDG PET, patients were instructed to fast for ≥12 hours, blood glucose levels were determined to ensure a level of <150 mg/dl, and unfractionated heparin was preadministered. Increased uptake of 67 Ga or 18 F-FDG in the myocardium that was higher than background activity was regarded as positive myocardial uptake. After the initiation of steroid treatment, 67 Ga scintigraphy or 18 F-FDG PET was repeated to evaluate the resolution of active myocardial inflammation. Echocardiography was performed by cardiologists. Left ventricular ejection fraction was calculated by the disc summation technique. Plasma B-type natriuretic peptide levels (normal, ≤18.4 pg/ml) and serum angiotensin-converting enzyme levels (normal, ≤21.4 IU/L) were measured.
Data are presented as mean ± SD for continuous variables and as numbers and percentages for categorical variables. Statistically significant differences were analyzed using Student’s t tests and Mann-Whitney U tests for continuous variables and chi-square tests for categorical variables. The event-free survival rate was estimated using Kaplan-Meier analysis, and the difference was analyzed using the log-rank test. Predictors of cardiac events in patients with high-degree AVB were analyzed using Cox proportional-hazard analysis. Variables for univariate analysis included age, gender, New York Heart Association functional class, the left ventricular ejection fraction, plasma B-type natriuretic peptide levels, and the initiation of steroid treatment. Variables with p values <0.10 in univariate analysis were entered into multivariate analysis. Hazard ratios are presented with 95% confidence intervals. Statistical analysis was performed with JMP version 8.0 (SAS Institute Inc., Cary, North Carolina), and significance was defined as p <0.05.
Results
Patient characteristics are listed in Table 1 . Twenty patients were diagnosed on the basis of histologic findings on endomyocardial biopsy, and the other 33 were diagnosed on the basis of clinical findings. Extracardiac organ involvements were observed in 43 patients, and the other 10 were classified as isolated cardiac sarcoidosis without extracardiac organ involvements. All 10 patients were diagnosed on the basis of histologic findings on endomyocardial biopsy that identified noncaseating epithelioid cell granulomas, but not necrosis or eosinophils.
| All (n = 53) | High-degree atrioventricular block (n = 22) | Ventricular tachyarrhythmia and/or heart failure (n = 31) | p | |
|---|---|---|---|---|
| Age (years) | 60 ± 13 | 60 ± 9 | 60 ± 15 | 0.948 |
| Female | 33 (62%) | 16 (73%) | 17 (55%) | 0.193 |
| Extracardiac organ involvements | 43 (81%) | 17 (77%) | 26 (84%) | 0.554 |
| Lung | 34 (64%) | 13 (59%) | 21 (68%) | 0.527 |
| Skin | 11 (21%) | 5 (27%) | 6 (19%) | 0.771 |
| Eye | 19 (36%) | 9 (41%) | 10 (32%) | 0.527 |
| Others | 10 (19%) | 4 (18%) | 10 (32%) | 0.475 |
| New York Heart Association functional class III or IV | 27 (51%) | 6 (27%) | 21 (68%) | 0.003 |
| Left ventricular end-diastolic diameter (mm) | 55 ± 9 | 51 ± 7 | 57 ± 9 | 0.013 |
| Left ventricular end-systolic diameter (mm) | 43 ± 11 | 38 ± 10 | 46 ± 11 | 0.005 |
| Left ventricular ejection fraction (%) | 42 ± 16 | 48 ± 15 | 38 ± 15 | 0.012 |
| Angiotensin-converting enzyme (IU/L) | 15.1 ± 7.0 | 16.0 ± 6.8 | 14.4 ± 7.2 | 0.438 |
| Log plasma B-type natriuretic peptide (pg/ml) | 2.34 ± 0.50 | 2.16 ± 0.43 | 2.46 ± 0.52 | 0.035 |
| Positive myocardial uptake of gallium-67 citrate or 18 F-fluoro-2-deoxyglucose | 40 (75%) | 19 (86%) | 21 (68%) | 0.125 |
| Diagnosis at the time of initial manifestation | 48 (91%) | 17 (77%) | 31 (100%) | 0.005 |
| Initiation of 30 or 40 mg prednisone daily | 42 (79%) | 17 (77%) | 25 (81%) | 0.771 |
| Medications after initial manifestation | ||||
| Beta-blockers | 33 (62%) | 7 (32%) | 26 (84%) | <0.001 |
| angiotensin-converting enzyme inhibitors/ angiotensin receptor blockers | 31 (58%) | 11 (50%) | 20 (65%) | 0.300 |
| Diuretics | 25 (47%) | 2 (9%) | 23 (74%) | <0.001 |
| Anti-arrhythmic drugs | 14 (26%) | 2 (9%) | 12 (39%) | 0.015 |
| Implantable cardioverter defibrillator | 12 (23%) | 1 (5%) | 11 (35%) | 0.007 |
| Cardiac resynchronization therapy with defibrillator | 9 (17%) | 1 (5%) | 8 (26%) | 0.043 |
| Median follow-up period (months) | 35 | 45 | 33 | 0.605 |
Among the 22 patients with high-degree AVB, complete AVB was observed in 20, and Mobitz II block was observed in 2. Pacemaker systems were implanted in 20 patients, ICDs were implanted in 1, and a cardiac resynchronization therapy device with a defibrillator was implanted in 1. Seventeen patients were treated with prednisone 30 or 40 mg/day, and the other 5 were not treated, because they were not diagnosed with cardiac sarcoidosis at the time of initial manifestation and were diagnosed at a later date. Among the 31 patients with VT and/or HF, ventricular fibrillation was observed in 1, and sustained VT was observed in 13. All patients were diagnosed with cardiac sarcoidosis at the time of initial manifestation. ICDs were implanted in 11 patients, and cardiac resynchronization therapy devices with defibrillators were implanted in 8. Twenty-five patients were treated with prednisone 30 or 40 mg/day, and the other 6 were not treated, because of the decisions of attending physicians or patient refusal.
As expected, HF and left ventricular dysfunction were less severe in patients with high-degree AVB than in those with VT and/or HF. Patients with high-degree AVB less often received ICDs or cardiac resynchronization therapy devices with defibrillators. There were no significant differences in age, positive myocardial uptake of 67 Ga or 18 F-FDG, and the initiation of steroid treatment between the 2 groups.
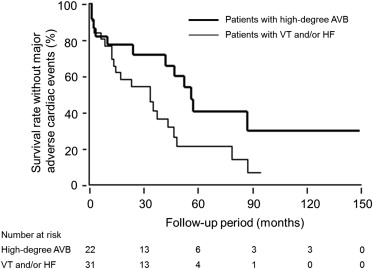
Over a median follow-up period of 34 months (range 1 to 149), major adverse cardiac events occurred in 34 patients. Of the 22 patients with high-degree AVB, 12 (55%) had major adverse cardiac events: 2 had ventricular fibrillation and were resuscitated by bystander cardiopulmonary resuscitation and an automated external defibrillator, 9 had sustained VT, and 1 was hospitalized for HF. After the first events, 1 patient died from HF. Of the 31 patients with VT and/or HF, 22 (71%) had major adverse cardiac events: 12 were hospitalized for HF, and 10 had sustained VT. After the first events, 6 patients died from VT and/or HF. Kaplan-Meier analysis showed that the survival rate without major adverse cardiac events was better in patients with high-degree AVB than in those with VT and/or HF (log-rank test, p = 0.046; Figure 1 ). However, this difference in the outcomes between the 2 groups was due mainly to the difference in the incidence of HF hospitalization. We compared the incidence of fatal cardiac events, which included cardiac death, ventricular fibrillation, and sustained VT, between patients with high-degree AVB and those with VT and/or HF. The survival rate without ventricular fibrillation or sustained VT was similar between the 2 groups (log-rank test, p = 0.877; Figure 2 ).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


