Early repolarization (ER) is typically observed in highly trained athletes as a physiologic consequence of increased vagal tone. The variant of anterior (V1 to V3) ER characterized by “domed” ST-segment elevation and negative T wave raises problems of differential diagnosis with the “coved-type” electrocardiographic pattern seen in Brugada syndrome (BS). This study was designed to identify electrocardiographic criteria for distinguishing athlete’s ER from BS. The study compared the electrocardiographic tracings of 61 healthy athletes (80% men, median age 23 ± 8 years), showing “domed” ST-segment elevation and negative T wave in leads V1 to V3, with those of 92 consecutive age- and sex-matched BS patients with a “coved-type” electrocardiographic pattern. The electrocardiographic analysis focused on the ST-segment elevation at J point (ST J ) and at 80 milliseconds after J point (ST 80 ). Athletes had a lower maximum amplitude of ST J (1.46 ± 0.7 vs 3.25 ± 0.6 mm, p <0.001) and lower ST J /ST 80 (0.8 ± 0.3 vs 1.6 ± 0.3, p <0.001). All patients (100%) with BS showed a downsloping ST-segment configuration (ST J /ST 80 >1) versus only 2 (3%) athletes (p <0.001). An upsloping ST-segment configuration (ST J /ST 80 <1) showed a sensitivity of 97%, a specificity of 100%, and a diagnostic accuracy of 98.7% for the diagnosis of ER. At multivariate analysis, ST J /ST 80 ratio remained the only independent predictor for ER (odds ratio 87, 95% confidence interval 19 to 357, p <0.001). In conclusion, the ST J /ST 80 ratio is a highly accurate electrocardiographic parameter for differential diagnosis between anterior ER of the athlete and BS. Our results may help in reducing the number of athletes who undergo expensive diagnostic workup or are unnecessarily disqualified from competition for changes that fall within the normal range of athlete’s heart.
This study was designed to compare the electrocardiographic pattern of athletes with an anterior early repolarization (ER) pattern characterized by domed ST-segment elevation followed by a negative T wave in leads V1 to V3 and patients with a coved-type Brugada electrocardiogram (ECG) to identify criteria for differential diagnosis.
Methods
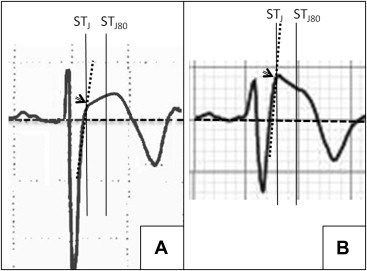
We included in the study 2 groups of subjects: (1) a consecutive series of 61 healthy endurance athletes who exhibited an anterior ER pattern characterized by domed ST-segment elevation and negative T wave at preparticipation electrocardiographic screening; (2) 92 consecutive age- and sex-matched patients with Brugada syndrome (BS) showing a type 1 Brugada ECG, defined as a coved ST-segment elevation ≥2 mm followed by negative T wave in at least 2 contiguous anterior (V1 to V3) leads, in the absence of any structural cardiac abnormalities. All BS patients exhibited a personal history of unexplained syncope, cardiac arrest because of documented ventricular fibrillation, symptomatic polymorphic ventricular tachycardia, and/or a family history of BS or premature sudden death. All athletes underwent a careful cardiovascular evaluation including history, physical examination, rest and exercise 12-lead ECG, and echocardiography, which excluded family history of sudden death, arrhythmic symptoms/syncope, and structural heart disease. Additional examinations, such as cardiac magnetic resonance, were prescribed in selected cases. Both athletes and patients with Brugada syndrome were at sinus rhythm and did not take any antiarrhythmic drugs or other drugs known to affect the QRS complex and/or ST segment/T wave. Athletes were evaluated by preparticipation screening yearly and had an uneventful outcome during a mean follow-up of 4 ± 2 years. ECGs were recorded on standard speed paper and digitally acquired. Each measurement was performed with digital calipers. The study focused on the following electrocardiographic parameters: (1) heart rate, (2) PR interval duration, (3) QRS duration, (4) presence of Sokolow-Lyon criteria for left ventricular hypertrophy (increased S wave in V1 + R wave in V5/V6 ≥35 mm), (5) corrected QT interval (QT C ) using the Bazzet’s formula, (6) ST-segment elevation at J point (ST J ) in the anterior lead (V1 to V3) with the greatest upward displacement of the ST segment, (7) ST-segment elevation at 80 milliseconds after J point (ST 80 ) in the lead V1 to V3 with the greatest upward displacement of the ST segment, and (8) ST J /ST 80 ratio. An ST J /ST 80 >1 identifies a downsloping ST segment, whereas an ST J /ST 80 <1 identifies an upsloping ST segment. When the offset of the QRS complex was difficult to define because of gradual slope toward the ST segment, the J point was extrapolated as the point at which the ST segment intersected the tangent of the slope of QRS terminal part extended upward ( Figure 1 ). Electrocardiographic interpretation was performed independently by 2 observers (AZ and FM): in case of disagreement, a third observer (DC) was consulted. All continuous variable values were reported as mean ± 1 SD and compared with the rank-sum test. Categorical variables were analyzed with the chi-square test or the Fisher’s exact test. Receiver operating characteristic curve analysis was used to evaluate the diagnostic accuracy of different ST J /ST 80 ratios for differentiating between BS and athlete’s ER. QRS interval duration, ST J , and ST J /ST 80 ratio were entered into a multivariate binary logistic regression analysis. A 2-tailed p <0.05 was considered statistically significant. All analyses were performed using SPSS 17 (SPSS Inc., Chicago, Illinois). The study protocol conformed to the ethical guidelines of the 1975 Declaration of Helsinki, and informed consent was obtained from each subject.
Results
The electrocardiographic findings of athletes and patients with BS are reported in Table 1 . Compared with patients with BS, athletes had a significantly lower heart rate, shorter QRS duration, and greater Sokolow index. With regard to ST-T repolarization parameters, athletes had a lower maximum amplitude of ST J and lower ST J /ST 80 ( Figure 2 ). No other electrocardiographic abnormalities were present. All patients (100%) with BS showed a downsloping ST-segment configuration versus only 2 athletes (3%, p <0.001). According to receiver operating characteristic curve analysis (area under curve = 0.98), a value of ST J /ST 80 <1 had a sensitivity of 97%, a specificity of 100%, and a diagnostic accuracy of 98.7% for ER. At multivariate analysis, ST J /ST 80 ratio remained an independent predictor for ER (odds ratio 87, 95% confidence interval 19 to 357, p <0.001), whereas QRS interval duration and maximum amplitude of the ST j point did not.
| Variable | Athletes (N=61) | Brugada patients (N=92) | P value |
|---|---|---|---|
| Men | 49 (80%) | 73 (79%) | 1.0 |
| Age (years) | 23±8 | 28±7 | 0.34 |
| Heart Rate (bpm) | 56±11 | 73±9 | <0.001 |
| PR interval (ms) | 160±31 | 181±32 | 0.043 |
| QRS interval (ms) | 91±0.14 | 112±0.21 | 0.01 |
| Sokolow-Lyon index (mm) | 36±8 | 29±11 | <0.001 |
| QTc interval (ms) | 399±32 | 387±44 | 0.87 |
| ST-segment elevation at J point (ST J ) (mm) ∗ | 1.46±0.7 | 3.25±0.6 | <0.001 |
| ST-segment elevation at 80 msec after J point (ST 80 ) (mm) ∗ | 1.87±1.1 | 2.1±0.3 | 0.53 |
| ST J /ST 80 Ratio ∗ | 0.8±0.3 | 1.6±0.3 | <0.001 |
| ST J /ST 80 Ratio >1 ∗ | 2 (3%) | 92 (100%) | <0.001 |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


