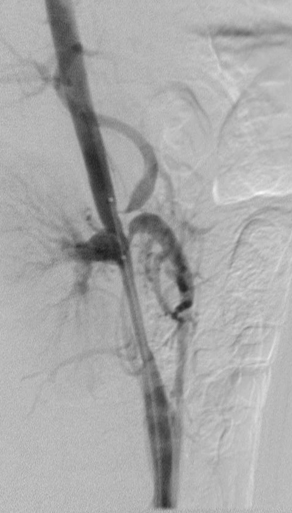
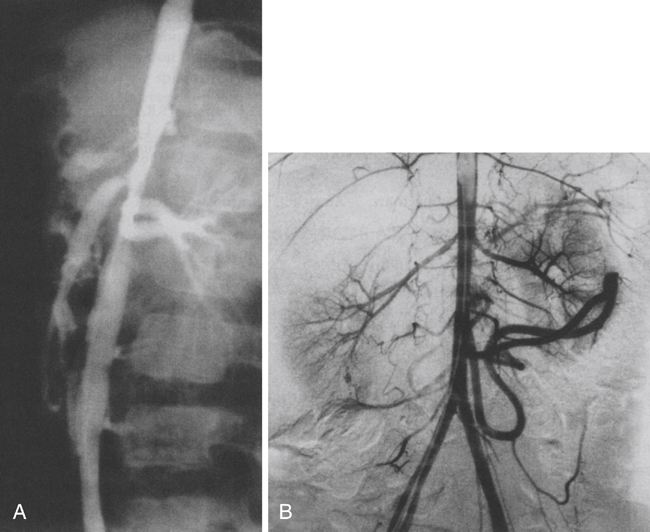
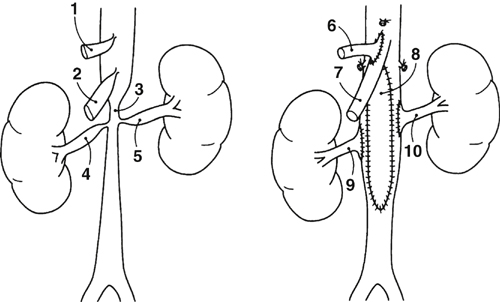
An occasional child has symptomatic intestinal ischemia manifest by postprandial abdominal pain and a failure to gain or maintain weight. The diagnosis in patients with suspected intestinal angina is most often confirmed by arteriographic imaging (Figures 1 and 2). The stenotic narrowings in these children invariably affect the ostia of the celiac and superior mesenteric arteries. The operative approach that we prefer is through a transverse supraumbilical abdominal incision with a left-sided medial visceral rotation and retroperitoneal exposure of the aorta from its diaphragmatic hiatus to its bifurcation. This incision is favored when performing a patch aortoplasty and splanchnic or renal reconstruction limited to the abdomen (Figure 3). A thoracoabdominal incision may be preferred in patients requiring an aortoaortic bypass originating from the supraceliac aorta (Figure 4). Care must be taken on retracting the left colon during these procedures, so as not to compromise blood flow through existing mesocolic collaterals originating from the inferior mesenteric artery. These collaterals provide critical blood flow to foregut and midgut structures. The specific type of splanchnic arterial reconstruction is dictated by the anatomic character of the disease affecting these vessels and the need for concomitant reconstructions of the aorta and renal arteries.
Operative Treatment of Pediatric Splanchnic Arterial Occlusive Disease
Clinical Presentation
Operative Therapy
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Thoracic Key
Fastest Thoracic Insight Engine