Figure 12.1
Single-stapler resection aided by a cotton peanut retracting the lung tissue toward the cartridge hinge

Figure 12.2
Trapezoidal resection, with the final stapling connecting both ends of the first two stapling lines, resulting in a trapezoidal lung parenchyma specimen
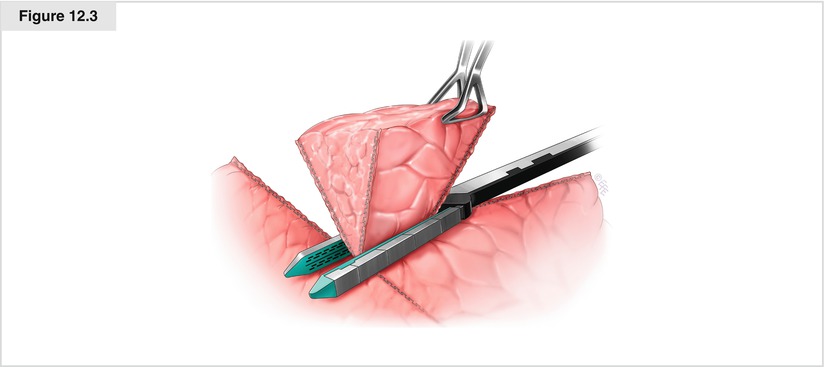
Figure 12.3
Parenchymal resection in a trigonal pyramid shape, with the pleural surface forming the base
Instruments
Cartridge length must be determined according to the staple length to be created. Cartridge color or thickness is selected based on the thickness and firmness of the parenchyma to be divided. If the parenchyma is too thin to secure air/blood tightness, air leakage/hemorrhage from the staple line may occur and suture closure may be necessary. If the parenchyma is too thick or firm even for green cartridges, segmentectomy or even lobectomy may be a better option. In marginal cases or in patients with fibrotic/emphysematous parenchyma, the visceral pleura right next to the staple lines may tear, requiring suture closure. This situation may be avoided by adding tissue reinforcement buttress materials such as Gore-Tex SeamGuard (W. L. Gore & Associates, Inc., Flagstaff, AZ) in stapling or by using cartridges preloaded with fully integrated buttress (Reinforced Reload; Covidien, Mansfield, MA). Although stapler approach is more flexible in open surgery than in VATS, it may be helpful to use articulating equipment even in an open procedure, so the lung parenchyma to be stapled is treated gently.
Indications in Lung Cancer
Sublobar resection, including wedge resection, is reportedly an acceptable alternative in patients with stage IA lung cancer and insufficient pulmonary reserve, when sufficient tumor-free margins are obtained (Kodama et al. 1997). Although there is still controversy regarding what constitutes “sufficient” margins (Fell and Kirby 2002), a margin greater than the maximum tumor diameter appears acceptable (Sawabata et al. 2004). Tumor-free margins must be confirmed intraoperatively, which may be achieved by the method described by Higashiyama et al. (2000). The used stapling cartridges are washed repeatedly with 50 ml of saline, which is then centrifuged. The sediment is stained by the Papanicolaou method and examined for cancer cells. This procedure is quick and less skill sensitive than pathologic examination. To reduce local recurrence following sublobar resection, the use of adjuvant iodine-125 brachytherapy may be considered (Pettiford et al. 2007).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


