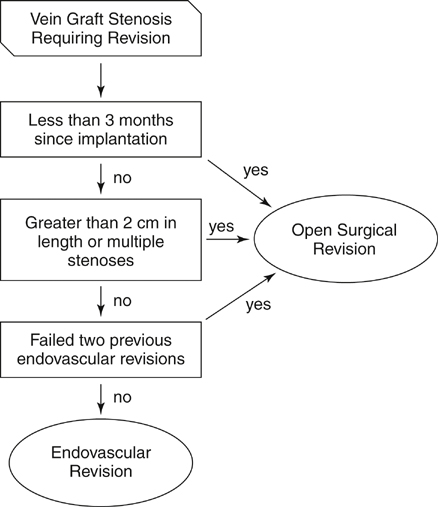
Open surgical revision can be adapted to encompass the full spectrum of potential graft pathologies, but the durability of endovascular treatments for the failing vein graft are inherently linked to the characteristics of the lesion. Time after implantation, lesion location, stenosis length, and graft occlusion have been identified as important surrogates for lesion pathology that significantly influence the intermediate and long-term success of endovascular interventions, and they thus become important factors in directing the choice between open and endovascular revision (Figure 1).
Open Surgery and Endovascular Management of Failing Infrainguinal Bypass Graft
Factors Influencing Repair Choice
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Thoracic Key
Fastest Thoracic Insight Engine