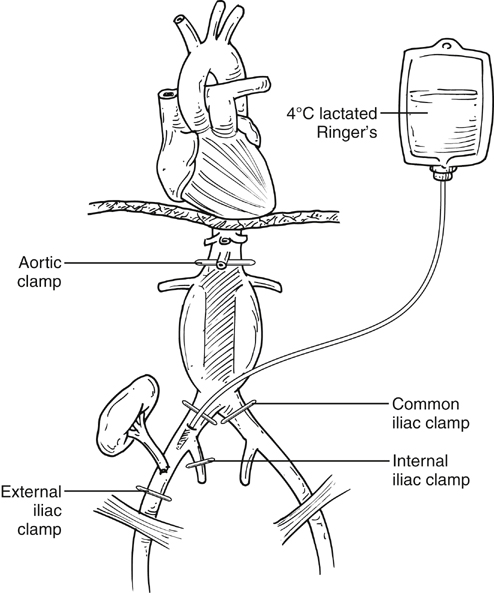
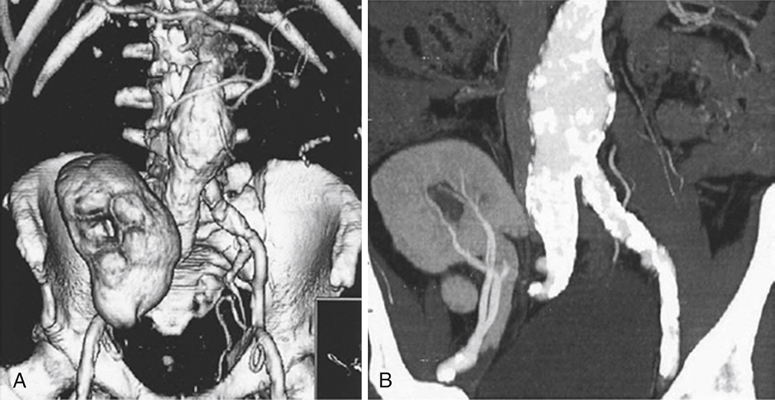
General principles of preoperative assessment apply with a focus on optimizing renal function before AAA repair. Aortoiliac imaging must be pursued cautiously, knowing that patients with compromised kidney function will be at increased risk for contrast-induced nephropathy. Patients with transplanted kidney and normal kidney function are usually able to tolerate iodinated contrast for arteriographic studies or computed tomography (CT) scans (Figure 1). Patients with suboptimal kidney function might require other means of contrast imaging. Magnetic resonance angiography (MRA) using gadolinium once was thought to be safer than standard iodinated contrast agents. However, several reports on nephrogenic systemic fibrosis have tempered enthusiasm for this agent. In open repair, aortic clamping results in decreased perfusion of the transplanted kidney, limited to flow originating from the lumbar, inferior mesenteric, and external iliac arteries. Intraoperative adjunctive renal protection measures can be done selectively, required only in patients with longer than 30 to 60 minutes of warm ischemia. However, some advocate renal protection in all patients, especially in those with impaired kidney function. Techniques of renal protection include a temporary shunt from the aorta to the iliac or femoral artery, temporary subclavian or axillofemoral shunt or bypass, in situ renal perfusion with a pump oxygenator by way of cannulation of the femoral vessels, in situ renal perfusion with cold solution through the common iliac artery, topical cooling, and general hypothermia. Even though shunting provides the kidney graft with steady blood perfusion, there is a risk of thromboembolization when cannulating atherosclerotic arteries, especially the proximal aorta. Furthermore, extracorporeal circulation increases the risk of hemorrhage and coagulopathy. Thus, selective hypothermia of the transplant by in situ perfusion with cold (4°C) Ringer’s lactate through the common iliac artery combined with topical cooling seems preferable (Figure 2). Explantation with temporary perfusion of the kidney followed by reimplantation has also been described, but it is complex and rarely required.
Open and Endovascular Repair of Abdominal Aortic Aneurysms in Kidney Transplant Patients
Renal Protection
Preoperative Measures
Intraoperative Techniques
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Open and Endovascular Repair of Abdominal Aortic Aneurysms in Kidney Transplant Patients