Disease or injury
DALYs (millions)
Total burden (%)
1
Lower respiratory tract infection
94.5
6.2
2
Diarrhea
72.8
4.8
3
Unipolar depression
65.5
4.3
4
Cardiac ischemia
62.6
4.1
5
HIV/AIDS
58.5
3.8
6
Encephalic vascular disease
46.6
3.1
7
Prematurity
44.3
2.9
8
Asphyxia and neonatal trauma
41.7
2.7
9
Traffic accidents
41.2
2.7
10
Neonatal infections
40.4
2.7
Predominant viruses in the respiratory system
Virus | Varieties: types, serotypes, genotypes, and other |
|---|---|
Rhinovirus | Species A, B, and C: >101 serotypes |
Coronavirus | Alpha: 229E, NL63; beta: OC43, HKU1, SARS, MERS |
Respiratory syncytial virus | A and B groups; genotypes and lineage |
Metapneumovirus | A and B groups; genotypes |
Adenovirus | 55 serotypes |
Influenza | Types A, B, and C; subtypes A H1–3, N1–2; several strains |
Parainfluenza | 4 serotypes |
Bocavirus | ? 1 serotype |
Others | Hantavirus, enterovirus, measles, chickenpox, cytomegalovirus |
These characteristics allow us to suspect specific causes of outbreaks or epidemics with reasonable certainty, considering associated clinical cases and detection of viruses at sentinel sites. Thus, a winter outbreak that involves infants under 1 year old and causes cases of obstructive bronchial illness will be due to RSV. A characteristic trait of influenza is an epidemic of disease that is marked by fever, cough, headache, and musculoskeletal aches, and that compromises preschool children, schoolchildren, and young adults. Parainfluenza virus outbreaks are associated with symptoms of hoarseness, gruffness, and cough, besides lower respiratory tract infections, in infants. Adenoviruses are feared because they sometimes cause intense feverish conditions and severe nosocomial infections.
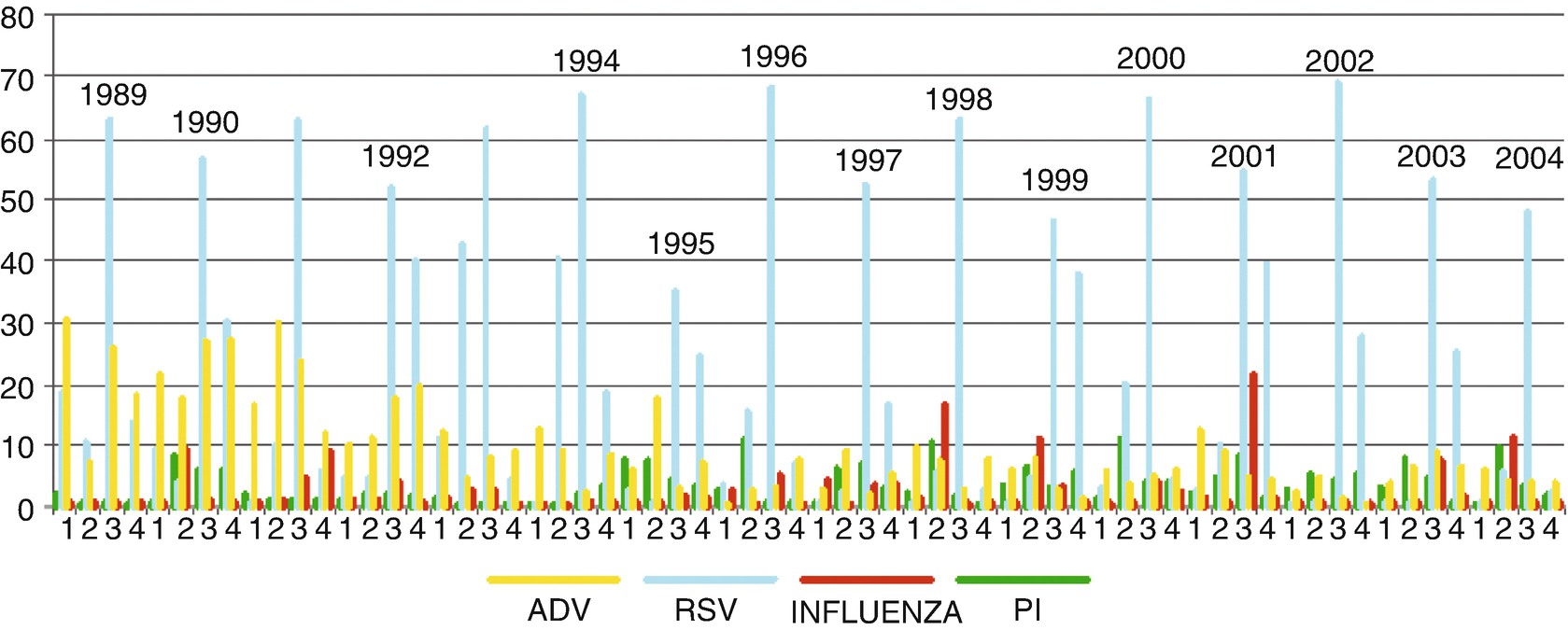
Viral monitoring at Hospital Roberto del Río (Santiago, Chile). Detection of respiratory viruses (adenovirus, RSV, influenza, and parainfluenza) by immunofluorescence in infants hospitalized for acute lower respiratory tract infection in 1989–2004
Viral respiratory infections are a very good example of a model of acute viral infection, in which viruses affect the individual, with or without symptoms, and then they leave him or her within a period of days or weeks. The course of infection depends on the interaction of various factors depending on: (1) the human host: age, immune status (based on previous infections and vaccinations), activity, tobacco use, etc.; (2) the virus: infecting dose, type, serotype, and viral strain; and (3) the environment: season, weather, humidity, contamination, geographical location, rural/urban setting, hospital/community, etc. From the host standpoint, acute respiratory infections are more frequent in childhood, particularly in infants and children under 2 years old, who represent the group with the biggest serious risk.
Diagnosis
Specific diagnosis of respiratory viruses is quite attainable nowadays because there are several immunodiagnostic techniques (immunofluorescence, enzyme-linked immunosorbent assay (ELISA), immunochromatography) available at public and private centers. They are easy to implement, with reasonably acceptable sensitivity and specificity, allowing appropriate study of cases that need it. Nowadays, molecular techniques (polymerase chain reaction (PCR) and reverse transcription PCR) are also available in many laboratories; they have high sensitivity and specificity, and provide results in less than 24 hours. The great sensitivity of these techniques enables detection of many agents, even in the same sample, raising questions about their interpretation. In severe cases or in deceased patients, they should always be implemented to establish the causes.
Emergent Infections
Among respiratory viruses, very good examples of “viral emergencies” are found, the most classic being the occurrence of global epidemics of influenza A virus derived from birds or pigs in 1918, 1957, 1968, and 2009; on these occasions, the virus broke through the species barrier and, thanks to multiple mutations, was able to transmit itself efficiently and establish itself as a “human virus.” A pandemic of severe acute respiratory syndrome (SARS) due to a coronavirus is another example of a phenomenon that has threatened the world and was able to be controlled. During August 2014, an outbreak of lower respiratory tract infections in children, associated with enterovirus D68, started in the USA, and its evolution is ongoing. Likewise, an emergency involving the Middle East respiratory syndrome (MERS) coronavirus (MERS-CoV) started in Saudi Arabia in 2012. Probably of animal origin (camels and bats) and transmissible through air, it has caused over 900 cases (30% lethal); luckily, it has not expanded efficiently in other territories.
Pathogeny of Viral Infections
Respiratory syndromes
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


