Figure 45.1
Positioning. The patient is placed in the supine position with both arms abducted at a 10° angle to minimize tension in the cervicothoracic crossing and brachial plexus. The contours of the pectoral muscle are clearly visible and allow free movement of the camera and introducer. The draping extends from the patient’s neck to below the navel line to expose the entire chest contour. To avoid an unnatural body shape, no back support is provided
Figure 45.2
Funnel chest analysis and implant position. The exact incision points through which to insert the pectus bar (Biomet Inc., Jacksonville, FL) into the chest are marked. Assessment of the strength and elasticity of the chest is recommended. The lower outer pectus point and inferior edge of the sternum are identified. With the sternal angle used as a reference, the second intercostal space (ICS) is identified as the highest possible pectus bar entry point. Excessive elevation of the upper chest segment may result in thoracic outlet syndrome. In female patients, it is essential to monitor for continued elevation post surgery, which may be caused by the strength of the pectus bar. Over- or undercorrection resulting from the method, as well as its optimal result, lies within a close range. Crucial factors are the implant length, the measurement from midaxillary line to midaxillary line using the template as a model minus 1 in., and shaping, that is, bending and molding of the pectus bar
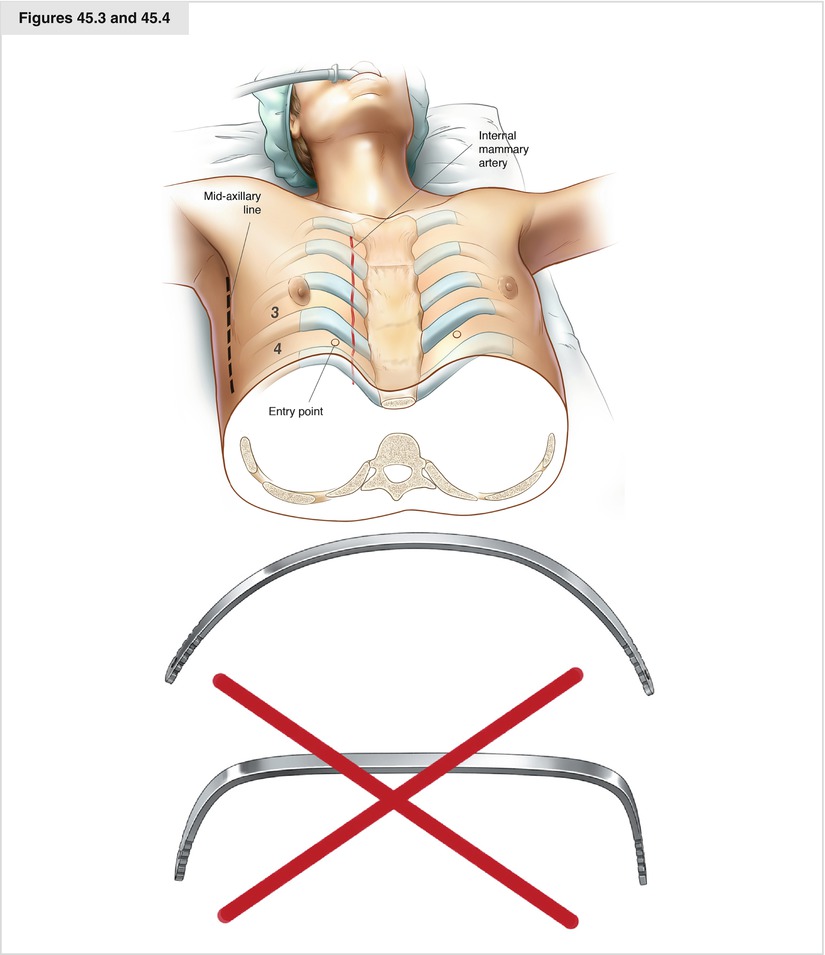
Figures 45.3 and 45.4
Input variables for the pectus bar’s shape. Input variables for the pectus bar’s shape are as follows:
1. Contours of the bar
2. Length of the bar
3. Points of entry and exit from the chest. It is important to analyze the correct biomechanical location, which will afford the greatest self-sustainability of the implant. Further, it is essential to analyze the length and rotation of the sternum, the position of the intercostal spaces, and the angulation of the costosternal connecting zone. The touch point of the pectus bar to the chest wall puts pressure on certain ribs, lowering that section of the chest. Thus, correction of the costal arches is affected and may even become impossible.
4. Number of implants, accounting for the patient’s degree of deformity, age, and gender
5. Differences between male and female contours
6. Analysis of the costal arch deformity
7. Incision type and location, taking surgical and aesthetic/cosmetic considerations into account
Figure 45.5




Guidance and control of the instruments. The camera is positioned from the right side via the sixth or seventh intercostal space in the anterior axillary line. Focus is on the diaphragm position. Gas pressure of 6- to 8 mm Hg shifts the lung and elevates the anterior chest wall. First, the mediastinal pleura is opened in the upper part at the end of the lower thymus horn directly retrosternally. From there, the incision is extended caudally retrosternally in full view of and protecting the pericardium. In cases of a low funnel and center-of-chest position of the heart, the pericardium may appear to be doubly present, causing the surgeon to pick the wrong incision point, which may lead to severe complications
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
