Chapter 2 Normal or Innocent Murmurs
Seven types of normal systolic murmurs and three types of normal continuous murmurs are known (Box 2-1).1 Normal systolic murmurs include the vibratory murmur, the main pulmonary artery murmur, the branch pulmonary artery murmur of the neonate, the supraclavicular systolic murmur, the systolic mammary souffle, the aortic systolic murmur of older adults, and the cardiorespiratory systolic murmur. All normal systolic murmurs are midsystolic, except the mammary souffle, and are not loudest at the right base.2 Normal continuous murmurs include the venous hum, the continuous mammary souffle, and the continuous cephalic (cranial) murmur (see Box 2-1).
Normal murmurs are never solely diastolic, with one exception—the transient left basal holodiastolic or middiastolic ductus arteriosus murmur, sometimes heard during the first 3 or 4 days of life.3 A valve-like structure at the pulmonary arterial end of the ductus (see Chapter 20) is responsible for selective diastolic flow.3,4
Normal systolic murmurs
Vibratory Systolic Murmur
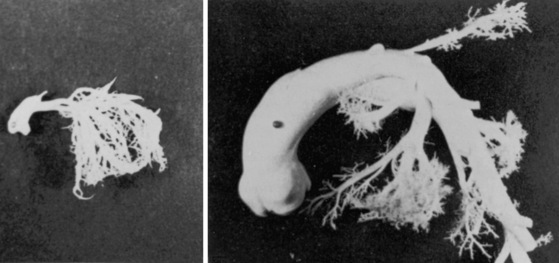
The normal vibratory midsystolic murmur was described by George F. Still in 1909 (Figures 2-1 and 2-2).5 Still wrote, “It is heard usually just below the level of the nipple, and about halfway between the left margin of the sternum and the vertical nipple line. … It’s characteristic feature is a twanging sound very like that made by twanging a piece of tense string. … Whatever may be it’s origin, I think it is clearly functional, that is to say, not due to any organic disease either congenital or acquired.”
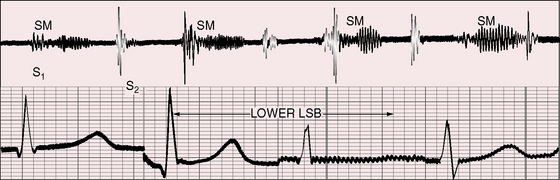
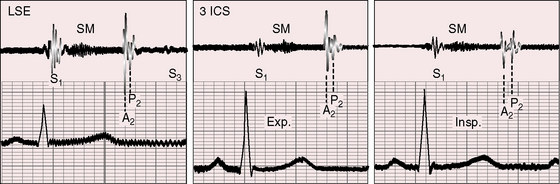
Still’s murmur is seldom heard in infants6 but is prevalent after age 3 years, with diminishing frequency toward adolescence.7,8–10 The murmur ranges from grade 1 to 3/6 and is loudest between the apex and lower left sternal edge in the supine position.9,11–14 During exercise, excitement, or fever, the murmur intensifies (see Figure 2-1).9 The quality is distinctive:9,15 vibratory or buzzing with a uniform, medium, pure frequency (70 to 130 cycles per second)16 that requires the stethoscopic bell for best assessment.11 The closest acoustic analogy is Still’s twanging of a taut rubber band or string (see previous quotation).17 The murmur begins shortly after the first heart sound and is typically confined to the first half of systole with a relatively long gap between the end of the murmur and the second heart sound (see Figures 2-1 and 2-2).
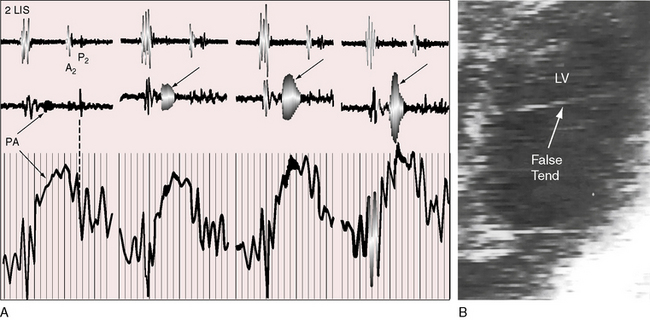
The mechanism of Still’s murmur remains to be established, but theories take into account the distinctive frequency composition and configuration, location on the chest wall, and incidence according to age. The pure medium frequency implies that a cardiac structure is set into periodic vibration during ventricular systole. Origin in the right side of the heart has been assigned to the pulmonary valve itself when “trigonoidation” of the leaflets results in periodic vibrations of the base of the cusps.10 A catheter across the pulmonary valve can tense the cusps and generate a transient pure-frequency midsystolic murmur (Figure 2-3A). The relatively low right ventricular ejection pressure and velocity are thought to cause the attachments of the pulmonary cusps to vibrate at a low to medium frequency. A murmur produced by a vibrating semilunar valve at its arterial attachment tends to be transmitted into the cavity of the concordant ventricle,2,18,19 which could account for the thoracic location of Still’s murmur between the apex and lower left sternal edge (i.e., topographically over the right ventricle). In children with Still’s murmur, Doppler echocardiocardiography has been used to identify systolic vibrations in the aortic valve and higher maximal acceleration of flow in the left ventricular outflow tract.14,20 However, a murmur that originates in a vibrating aortic valve is transmitted into the left ventricular cavity and heard best over the left ventricular impulse. Midsystolic murmurs in adults have been ascribed to high intraventricular velocities generated by vigorous left ventricular contraction associated with an increase in left ventricular mass.21 Origin of Still’s murmur has also been assigned to the left ventricular cavity, a location that is in accord with delayed response to the Valsalva’s maneuver.22 Left ventricular bands or false tendons (Figure 2-3B) are thought to vibrate periodically during ventricular systole and transmit their vibrations to the chest wall.23–25 A high percentage of patients with Still’s murmur reportedly have left ventricular bands, especially in the outflow tract.23–26 However, the prevalence rate of Still’s murmur declines from childhood to adolescence,9,10 whereas the prevalence rate of left ventricular bands is the same in children, adolescents, and adults.23,24,27 The incidence rate of Still’s murmur is thought to exceed the incidence rate of left ventricular bands,14 although incidence rate depends largely on the avidity with which bands are sought with echocardiography.
Pulmonary Artery Systolic Murmur
The normal systolic murmur in the main pulmonary artery is most prevalent in children, adolescents, and young adults.9,11,28 The murmur is midsystolic with maximal intensity in the second left intercostal space next to the sternum (Figure 2-4) and ranges from bare audibility to grade 3/6 in response to exercise, fever, or excitement. The frequency composition is medium pitched and impure, best heard in the supine position with the stethoscopic diaphragm or moderate pressure of the bell during full held exhalation.9,11,29 The murmur represents normal ejection vibrations that reach the threshold of audibility from within the main pulmonary artery during right ventricular systole. The chest wall location is appropriate for origin in the pulmonary trunk, and intracardiac phonocardiograms record midsystolic murmurs within the pulmonary trunk in healthy young subjects.29
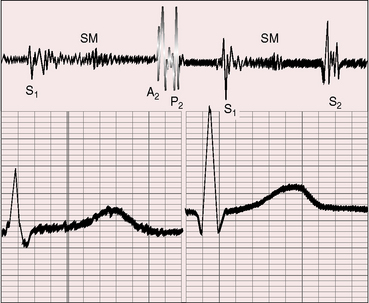
These murmurs are commonly heard during pregnancy and in subjects with anemia or hyperthyroidism. Loss of thoracic kyphosis increases proximity of the pulmonary trunk to the chest wall and increases the incidence rate of pulmonary systolic murmurs in the second left interspace.30
Branch Pulmonary Artery Systolic Murmur
Branch pulmonary artery systolic murmurs are occasionally heard in healthy neonates, especially premature neonates.28,31–33 These murmurs are typically grade 1 to 2/6 and are medium pitched and impure but most importantly, are distributed to the left and right anterior chest, axillae, and back. The similarity of frequency composition to breath sounds, the rapid respiratory rate of infants, and the widespread thoracic locations of pulmonary artery systolic murmurs cause these murmurs to be overlooked. Audibility is improved if respiration is temporarily arrested with pinching the nostrils while the infant sucks a pacifier. Auscultation is best carried out with examination of the infant in both supine and prone positions and with use of the stethoscopic diaphragm applied to the right and left anterior chest, back, and axillae. The murmurs are typically confined to neonates, are usually absent at the first well-baby examination, and seldom persist beyond 3 to 6 months of age.13,28,34 The transient branch pulmonary artery systolic murmur in healthy neonates is indistinguishable from the peripheral murmur of fixed stenosis of the pulmonary artery and its branches (see Chapter 10). The analogy sheds light on the mechanism of production.28,32,33 The pulmonary trunk in the fetus is a relatively dilated domed structure because it receives the output of the high-pressure right ventricle. Proximal right and left pulmonary arteries arise from the pulmonary trunk as comparatively small lateral branches that receive a paucity of intrauterine blood flow. When the lungs expand at birth, the difference in size between the pulmonary trunk and its right and left branches transiently persists, especially in premature infants (Figure 2-5).34 In addition to the disparity in size, the branches arise at relatively sharp angles from the inferior and posterior walls of the pulmonary trunk. These anatomic arrangements account for both the turbulence and the physiologic drop in systolic pressure from pulmonary trunk to proximal branches and for the branch pulmonary artery systolic murmur.28,33
Supraclavicular Systolic Murmur
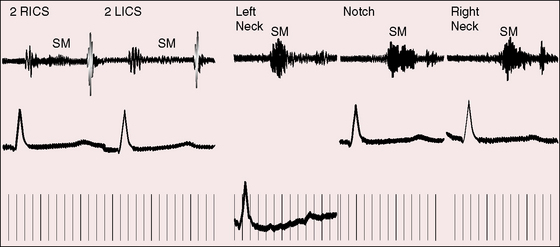
Normal supraclavicular systolic arterial murmurs are typically heard in children and young adults, are always maximal above the clavicles, tend to be louder on the right, are generally bilateral, and are prominent in the suprasternal notch (Figure 2-6).2,35 The weight of evidence assigns supraclavicular systolic murmurs to the aortic origins of major brachiocephalic arteries, especially the subclavians.36 Intensity can reach grade 4/6, may generate a thrill, and may be sufficient for radiation below the clavicles but with distinct attenuation (see Figure 2-6). The configuration of the supraclavicular systolic murmur is crescendo-decrescendo, the onset is abrupt, the duration is brief, and the timing is maximal in the first half or two thirds of systole (see Figure 2-6). The frequency composition is uneven, but the murmur is seldom noisy even when loud. Partial compression of the subclavian artery intensifies the murmur, whereas compression sufficient to obliterate the ipsilateral radial pulse has the opposite effect. Auscultation is most effectively carried out when the patient is sitting upright and looking straight ahead with shoulders relaxed and forearms and hands on the lap (Figure 2-7A).2,37 The stethoscopic bell is applied above the medial aspect of the right clavicle. The shoulders are then hyperextended, with elbows brought sharply behind the back until shoulder girdle muscles are taut (Figure 2-7B). When this maneuver is done smoothly but rapidly, the supraclavicular murmur diminishes considerably or disappears altogether.37
< div class='tao-gold-member'>
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


