Nonseminomatous Germ Cell Tumor
Presentation
A 27-year-old student is admitted to the hospital complaining of dyspnea and cough occurring over the past 6 weeks. The patient has no significant medical problems and does not smoke. He has no family history of malignancy. He has not traveled outside the United States in 20 years. On physical examination, vital signs are stable, heart sounds are normal, and there are decreased breath sounds over the right chest.
▪ Chest X-rays
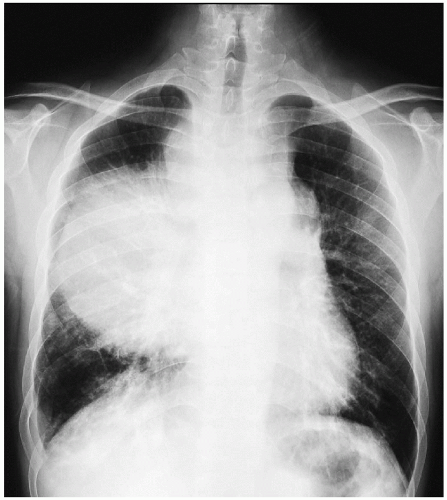 Figure 1-1 |
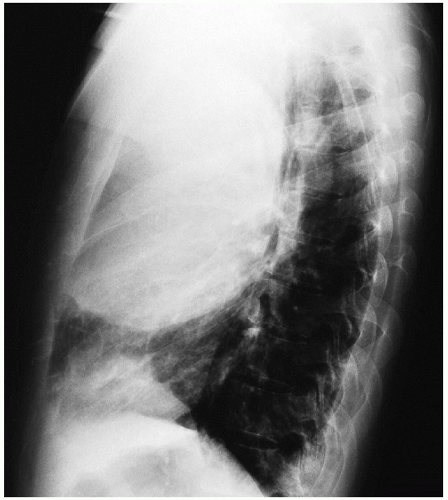 Figure 1-2 |
Chest X-ray Report
The chest x-rays demonstrate a large anterior mass located in the mediastinum and the right chest. The heart is not enlarged. There are no pleural effusions. There are no masses in the left lung field.
Discussion
The differential diagnosis of anterior mediastinal masses includes thymoma, lymphoma, thyroid goiter, and germ cell tumor. In a patient who presents with an anterior mediastinal mass, a complete history and physical examination is important. A history of ptosis, dysarthria, and muscle weakness, particularly if the weakness increases with increased activity, suggests the diagnosis of mediastinal thymoma associated with myasthenia gravis. Patients with enlarged axillary, supraclavicular, and cervical lymph nodes may have lymphoma. About 60% of patients with mediastinal germ cell tumors are asymptomatic, and 40% have dyspnea and chest pain.
In a young man with a mediastinaltumor, a computed tomography (CT) scan of the chest, as well as tumor markers, should be obtained. Tumor markers include α-fetoprotein, β-human chorionic gonadotropin, and lactate dehydrogenase.
▪ CT Scans
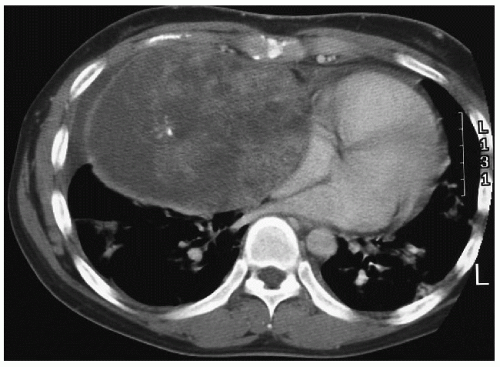 Figure 1-3 |
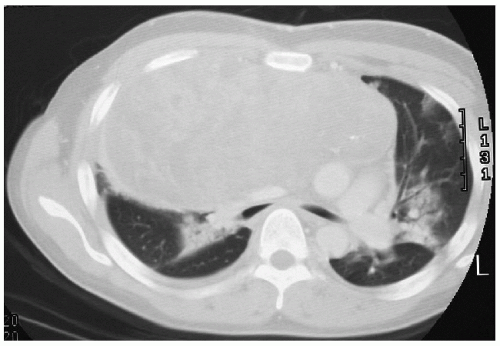 Figure 1-4 |
CT Scan Report
The chest CT demonstrates a heterogeneous 18-cm × 8-cm × 9.8-cm mass with calcifications and multiple areas of necrosis and hemorrhage. The mass extends into the neck and right pleural space. There is compression of the trachea and both main-stem bronchi.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


