Noninvasive Ventilation
GENERAL PRINCIPLES
• Noninvasive ventilation (NIV) or noninvasive positive pressure ventilation refers to the use of a mask or similar device to provide ventilatory support.
• This definition is broad and could include external negative pressure devices (e.g., the “iron lung,” historically used for ventilation of patients suffering from poliomyelitis-induced paralysis), cuirass ventilation (external shell with applied negative pressure), and rocking beds—an effective means to ventilate a patient with bilateral diaphragmatic paralysis.
• NIV by definition excludes any modality that bypasses the upper airway, such as laryngeal masks, endotracheal intubation, or tracheostomy.
• For the purposes of this chapter, NIV refers to mechanical ventilatory support delivered through a face mask, nasal mask, or similar device.
CLASSIFICATION
• Invasive mechanical ventilation and NIV have similar physiologic principles.
• The modes of ventilatory support (i.e., the way in which the ventilator triggers, delivers, and ends the breath) are similar to invasive mechanical ventilation. However, there is no standardization between manufacturers regarding mode terminology.
• Two of the most commonly encountered modes include continuous positive airway pressure (CPAP) and bilevel positive airway pressure (BiPAP).
Continuous Positive Airway Pressure
• CPAP maintains a set positive pressure throughout the respiratory cycle (inhalation and exhalation) and is not ventilatory support in a strict physiologic sense.
• CPAP “stents open” the upper airway with continuous pressure. This concept helps explain the utility of CPAP in disorders such as obstructive sleep apnea but does not explain why a treatment that does not provide ventilatory support can be of use in the patient who is suffering from hypoxemic or hypercapnic respiratory failure.
• Clinical applications include:
 Hypoxemic respiratory failure
Hypoxemic respiratory failure
 Increases partial pressure of oxygen in the alveoli. In the alveolar gas equation, PAO2 = FiO2 (PB – 47) – 1.2 (PaCO2), if PB is barometric pressure (or in our case, the pressure delivered from the ventilator through the mask), an increase in the mean airway pressure throughout the respiratory cycle for a given fraction of inspired oxygen (FiO2) will increase the partial pressure of inspiratory oxygen and therefore oxygen tension in the alveoli (PAO2).
Increases partial pressure of oxygen in the alveoli. In the alveolar gas equation, PAO2 = FiO2 (PB – 47) – 1.2 (PaCO2), if PB is barometric pressure (or in our case, the pressure delivered from the ventilator through the mask), an increase in the mean airway pressure throughout the respiratory cycle for a given fraction of inspired oxygen (FiO2) will increase the partial pressure of inspiratory oxygen and therefore oxygen tension in the alveoli (PAO2).
 Provides extrinsic positive end-expiratory pressure (PEEP). It recruits the underventilated or collapsed lung, probably by preventing alveolar collapse during exhalation.
Provides extrinsic positive end-expiratory pressure (PEEP). It recruits the underventilated or collapsed lung, probably by preventing alveolar collapse during exhalation.
 Hypercapnic respiratory failure can decrease the work of breathing, by overcoming intrinsic PEEP in patients with chronic obstructive airway disease.
Hypercapnic respiratory failure can decrease the work of breathing, by overcoming intrinsic PEEP in patients with chronic obstructive airway disease.
 In advanced chronic obstructive pulmonary disease (COPD) with hyperinflation, airflow obstruction and decreased elastic recoil lead to a prolonged expiratory phase. In respiratory distress, inspiration may occur before expiration is completed, leading to dynamic hyperinflation.
In advanced chronic obstructive pulmonary disease (COPD) with hyperinflation, airflow obstruction and decreased elastic recoil lead to a prolonged expiratory phase. In respiratory distress, inspiration may occur before expiration is completed, leading to dynamic hyperinflation.
 Ineffective ventilation and increasing work of breathing cause the buildup of carbon dioxide and worsening respiratory acidosis. The positive elastic recoil pressure left behind in this hyperinflated patient at the end of expiration is termed intrinsic PEEP.
Ineffective ventilation and increasing work of breathing cause the buildup of carbon dioxide and worsening respiratory acidosis. The positive elastic recoil pressure left behind in this hyperinflated patient at the end of expiration is termed intrinsic PEEP.
 Delivering PEEP via CPAP lessens the work of breathing by overcoming intrinsic PEEP. In intubated patients with acute respiratory failure, extrinsic PEEP (PEEPe) has been demonstrated to reduce the work of breathing by 50%. The same principle applies to the noninvasively ventilated patient.
Delivering PEEP via CPAP lessens the work of breathing by overcoming intrinsic PEEP. In intubated patients with acute respiratory failure, extrinsic PEEP (PEEPe) has been demonstrated to reduce the work of breathing by 50%. The same principle applies to the noninvasively ventilated patient.
Bilevel Positive Airway Pressure
• BiPAP is CPAP with a second level of pressure support during inspiration, akin to pressure support ventilation for mechanically ventilated patients.
• In practical terms, BiPAP requires the operator to set two variables, inspiratory positive airway pressure (IPAP) and expiratory positive airway pressure (EPAP), that are measured in cm H2O.
 IPAP is the ventilatory pressure support the patient receives when either the machine or the patient initiates a breath.
IPAP is the ventilatory pressure support the patient receives when either the machine or the patient initiates a breath.
 EPAP is the pressure against which the patient exhales at the termination of inhalation.
EPAP is the pressure against which the patient exhales at the termination of inhalation.
 “Initial settings” are often referred to by the IPAP followed by the EPAP (e.g., 12 cm H2O and 5 cm H2O).
“Initial settings” are often referred to by the IPAP followed by the EPAP (e.g., 12 cm H2O and 5 cm H2O).
 The greater the difference between the IPAP and the EPAP, the greater the theoretical ventilatory support the patient receives.
The greater the difference between the IPAP and the EPAP, the greater the theoretical ventilatory support the patient receives.
 However, progressively higher levels of EPAP and IPAP are not usually well tolerated by the patient, and as with any initiation of NIV, the patient should be observed closely to see if effective patient–ventilator synchrony occurs.
However, progressively higher levels of EPAP and IPAP are not usually well tolerated by the patient, and as with any initiation of NIV, the patient should be observed closely to see if effective patient–ventilator synchrony occurs.
SPECIFIC DISEASE INDICATIONS FOR NONINVASIVE VENTILATION
• NIV may improve outcomes by avoiding intubation and the attendant risks of secondary infections in this patient population.
• In general, NIV is most effective in patients with cardiogenic pulmonary edema, patients with hypercapnic respiratory failure, and in weaning patients from invasive mechanical ventilation.
Cardiogenic Pulmonary Edema
• NIV helps to unload the respiratory muscles in respiratory failure caused by heart failure and pulmonary edema and improves cardiac performance by reducing right and left ventricular preload and mean transmural filling pressures.
• CPAP is recommended for hypoxemic patients with cardiogenic pulmonary edema who remain hypoxemic despite maximal medical therapy.
• A recent meta-analysis pooled the results of 34 trials in patients with acute cardiogenic pulmonary edema confirmed an overall mortality benefit utilizing NIV (both CPAP or bilevel modes), as well as a reduction in the risk of intubation.1
• Noninvasive methods of respiratory support should not be used in hemodynamically unstable patients or in those with ongoing cardiac ischemia.
Chronic Obstructive Pulmonary Disease
• NIV can be an effective initial respiratory support modality in the setting of acute COPD exacerbation. Studies have shown improvements in pH, PCO2, and respiratory rate, and lower intubation rates and lower mortality when compared to standard therapy.2,3
 NIV should be considered in patients with acute exacerbations of COPD in whom a respiratory acidosis persists (pH <7.35) despite maximum medical therapy. In a multicenter randomized controlled trial of BiPAP via nasal or face mask with standard therapy (n = 236 patients), NIV reduced the need for intubation and rate of in-hospital mortality was significantly reduced compared to the standard therapy group.
NIV should be considered in patients with acute exacerbations of COPD in whom a respiratory acidosis persists (pH <7.35) despite maximum medical therapy. In a multicenter randomized controlled trial of BiPAP via nasal or face mask with standard therapy (n = 236 patients), NIV reduced the need for intubation and rate of in-hospital mortality was significantly reduced compared to the standard therapy group.
 NIV helps to decrease the need for invasive mechanical ventilation. Between 1998 and 2008 in the United States, NIV use increased from about 1% to 4.5% of all patients admitted with COPD exacerbations, and invasive ventilation dropped from 6% to 3.5% accordingly. Similarly, patients who fail NIV and require intubation have a much higher mortality.4
NIV helps to decrease the need for invasive mechanical ventilation. Between 1998 and 2008 in the United States, NIV use increased from about 1% to 4.5% of all patients admitted with COPD exacerbations, and invasive ventilation dropped from 6% to 3.5% accordingly. Similarly, patients who fail NIV and require intubation have a much higher mortality.4
• NIV can also facilitate weaning and extubation of COPD patients from invasive mechanical ventilation. Randomized trials in this population of patients have shown shorter durations of intubation, lower rates of nosocomial pneumonia, shorter hospital stays, and improved survival.5
Postextubation Respiratory Failure
• Most of the benefit of NIV in postextubation respiratory failure applies to hypercapnic patients who may benefit from a trial of NIV and close monitoring.
• In most cases, reintubation is more prudent and helps to prevent situations of emergent reintubation from a failure of trial of NIV.
Chest Wall Deformity and Neuromuscular Disease
• NIV can be an appropriate first-line choice in patients with acute and acute-on-chronic respiratory failure.
• In our experience at Washington University, these patients often do better in the long term with NIV that delivers a fixed tidal volume using laptop ventilators in assist control (AC), synchronized intermittent mandatory ventilation (SIMV), or even newer modes of average volume assured pressure support (AVAPS).
 With bilevel pressure ventilation, tidal volume and minute ventilation may decrease with disease progression.
With bilevel pressure ventilation, tidal volume and minute ventilation may decrease with disease progression.
 Similarly, acute changes in lung compliance due to alveolar consolidation due to pneumonia may render pressure-based NIV inadequate.
Similarly, acute changes in lung compliance due to alveolar consolidation due to pneumonia may render pressure-based NIV inadequate.
Trauma Patients
• CPAP can be considered in patients with chest wall trauma who remain hypoxemic despite regional anesthesia.
• Several small randomized, controlled trials support using CPAP for patients with isolated chest trauma, rib fractures, and hypoxemia.6,7
• Standard mechanical ventilation should still be used in patients with greater than moderate lung injury (defined by a PaO2 of <60 mm Hg on an FiO2 of ≥40%), as these patients were excluded from the study. Furthermore, the injury severity score was higher in the intubated group.6
Acute Hypoxemic Respiratory Failure and Pneumonia
• The use of NIV in hypoxemic respiratory failure is less clear than in the above disorders and depends on the severity of disease.
• The current recommendation is that NIV can be used as an alternative to endotracheal intubation in carefully selected patients with acute hypoxemic respiratory failure with recognition that many of these patients may require intubation and if NIV is chosen, the patient should be intubated if not improving within 1–2 hours of initiation.
Asthma
• Routine use of NIV is not recommended.
• Severe respiratory acidosis in the setting of an acute asthma exacerbation should be treated with intubation and invasive ventilation.
Palliative Noninvasive Ventilation
• NIV has the potential to alleviate dyspnea in end-of-life circumstances.8
• Use of NIV should be weighed with issues of discomfort and claustrophobia from face–mask ventilation. Effective communication and clarification of the goals of care need to occur and managed on a case-by-case basis.
INITIATION OF NONINVASIVE VENTILATION
• NIV is best used for patients with:
 High PaCO2 (pH range of 7.25–7.35)
High PaCO2 (pH range of 7.25–7.35)
 Low alveolar–arterial oxygen gradient
Low alveolar–arterial oxygen gradient
 A good level of consciousness and cooperation
A good level of consciousness and cooperation
• NIV should only be initiated in locations with experienced staff, including respiratory therapists who are immediately available. In practice, this tends to restrict NIV to intensive care units (ICUs) or a designated respiratory ward.
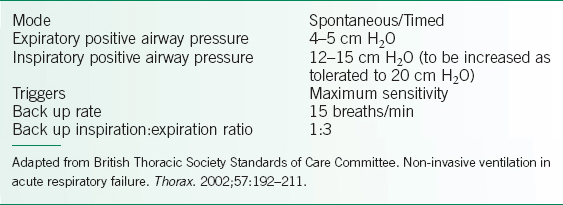
• For initial settings see Table 6-1.9
 IPAP
IPAP
 EPAP
EPAP
 FiO2: this may be from a flow rate of O2 L/min or from direct FiO2 setting.
FiO2: this may be from a flow rate of O2 L/min or from direct FiO2 setting.
 In some models, high flow rates may become uncomfortable and can lead to ventilator dyssynchrony.
In some models, high flow rates may become uncomfortable and can lead to ventilator dyssynchrony.
 Newer ventilators use an oxygen mixer that allows for titration of FiO2 before its entry into the circuit without adjusting the flow rate. This setup is subsequently more comfortable for the patient and more beneficial for ventilation.
Newer ventilators use an oxygen mixer that allows for titration of FiO2 before its entry into the circuit without adjusting the flow rate. This setup is subsequently more comfortable for the patient and more beneficial for ventilation.
TABLE 6-1 TYPICAL INITIAL VENTILATOR SETTINGS FOR BILEVEL POSITIVE AIRWAY PRESSURE IN A PATIENT WITH ACUTE HYPERCAPNIC RESPIRATORY FAILURE DUE TO COPD
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


