Non-Small Cell Lung Carcinoma Evaluation of Pleural and Vascular Invasion, Resection Margins, and Treatment Effect
Allen Burke, M.D.
Fabio Tavora, M.D., Ph.D.
Borislav A. Alexiev, M.D.
Pleural Invasion
Histologic Assessment
Invasion into the pleura is a routine assessment for non-small cell lung carcinomas, which is required for tumor staging (see Chapter 73). The extent of invasion has been classified into fibrous tissue under the pleura without invasion of the elastic tissue (PL0), invasion of visceral pleural elastic tissue (PL1), invasion of parietal pleura (PL2), and invasion through parietal pleura (PL3). PL1 or PL2 denotes pT2 stage, and PL3 is equivalent to chest wall invasion (pT3).1 Therefore, the distinction between invasion of visceral and parietal pleura, which is difficult, is not necessary. When there is chest wall invasion, there is typically resection of ribs (Fig. 87.1).
Invasion into the pleura is often suspected grossly by retraction of the surface.2 Invasion into the chest wall is generally evident upon reading the operative note and will result in chest wall fat or rib resection. In these cases, it is important to ink the specimen in order to obtain chest wall margins. If the pleura is intact and no chest wall has been removed, inking the pleural surface is unnecessary and may interfere with the microscopic evaluation of tumor invasion. It is important in this context to remember that the visceral pleura is not a surgical margin and that parietal pleura is resected only if there is chest wall invasion.
Use of Elastic Stains
Elastic stains highlight the pleural elastic tissue, which is helpful in assessing invasion, as penetration of the elastic layer is considered the basis for upstaging the tumor to pT2. The elastic lamina appears as a black serpentine band of interconnecting fibers beneath the mesothelial layer. The pleural visceral layer is usually accentuated in areas of invasion, with a fibroblastic reaction and reaction of the elastic layer into the lung parenchyma3 (Figs. 87.2 and 87.3).
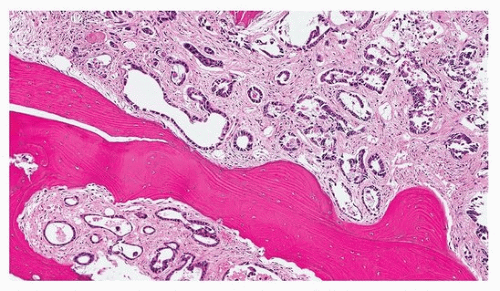 FIGURE 87.1 ▲ Invasion into the chest wall. If there is PL3 invasion, portions of the chest wall (fat, fascia, skeletal muscle or bone) will be removed, necessitating additional margin evaluation. In this case, tumor invaded the bone. |
Taube et al. demonstrated that 17% of adenocarcinomas and 26% of squamous carcinomas that were judged as negative for pleural invasion on hematoxylin-eosin staining were upstaged from pT1 to pT2 tumors after review of elastic stains (Movat pentachrome stains).3 These findings have led to the recommendation that all pT1 tumors that abut the pleura microscopically be stained for elastic tissue, Verhoeff elastic van Gieson stain, elastin hematoxylin and eosin, Weigert elastic stain, or Movat pentachrome stains.1
Adenocarcinoma in situ or minimally invasive adenocarcinomas by definition do not invade the pleura. Also by definition, the lepidic growth pattern of adenocarcinomas does not invade the pleural elastic tissue.3
Prognostic Implications
Overall, pleural invasion is identified in about 25% of resected lung cancers1 although in some series the number is far higher.4 Over half of lung tumors that have grossly puckered pleural surfaces show pleural invasion histologically using elastic stains.2 Pleural invasion is associated tumor size >3 cm, higher tumor grade, vascular invasion,
mediastinal lymph node metastasis, extranodal involvement, and higher stage.2 In one study, the 5-year survival of patients with and without pleural invasion was 57.9% and 83.0%, respectively, justifying its use in pathologic staging.2 Another study showed that visceral pleural and lymphovascular invasion were poor prognostic factors and that perineural invasion had no effect on survival.4
mediastinal lymph node metastasis, extranodal involvement, and higher stage.2 In one study, the 5-year survival of patients with and without pleural invasion was 57.9% and 83.0%, respectively, justifying its use in pathologic staging.2 Another study showed that visceral pleural and lymphovascular invasion were poor prognostic factors and that perineural invasion had no effect on survival.4
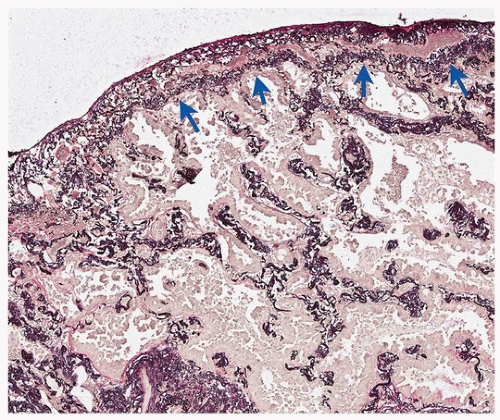 FIGURE 87.2 ▲ No pleural invasion, elastic stain. The elastic layer is intact (arrows). The tumor cells are pale tan-brown and barely visible. |
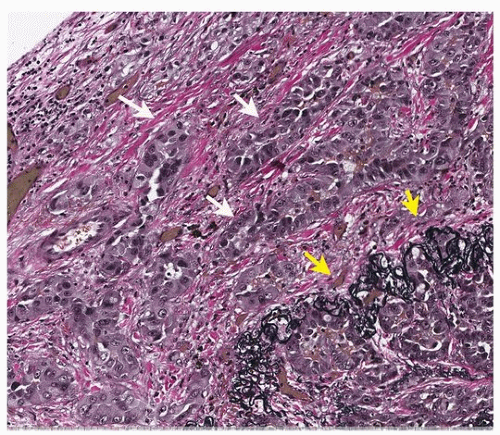 FIGURE 87.3 ▲ With elastic staining, tumor can be seen outside the elastic layer of the pleura (arrows). |
Nitadori et al. showed that pleural invasion in peripheral adenocarcinomas ≤2 cm did not affect survival or risk of recurrence, but affected both survival and recurrence only in tumors that were 2 to 3 cm.5 Current guidelines, however, still recommend grouping all tumors <3 cm as stage pT2a if there is pleural involvement.
Lymphovascular Invasion
General
The acronym “LVI” was initially applied to “lymphatic vessel invasion” and did not denote blood vessel invasion.6 Currently, however, LVI frequently refers to “lymphovascular invasion,” a term that the College of American Pathologists (CAP) uses for both blood vessel and lymphatic invasion. A synonym is “angiolymphatic invasion,” which combines blood vessel and lymphatic invasion.7 The term “lymphatic permeation” is sometimes used for lymphatic invasion, and “vascular invasion” generally denotes blood vessel invasion.8
In the current CAP checklist, the type of invasion (blood vessel vs. lymphatic) is not specified. Lymphatic or blood vessel invasion does not affect the stage of the tumor, unlike pleural invasion.
Lymphatic Invasion
Lymphatic invasion occurs in 13% to 59% of non-small cell lung carcinomas. There is no association with squamous or adenocarcinoma subtypes.6,7,8,9 Lymphatics most frequently are seen surrounding arteries (Fig. 87.4) or airways.
Lymphatic invasion is more frequent in tumors with lymph node metastases and advanced stage, but not with the presence of distant metastasis.6 There is a weakly significant association with blood vessel invasion.7 In conjunction with blood vessel invasion, there is an association with size between 2 and 3 cm, standard uptake value (SUV) on positron emission tomography (PET) scans, pleural invasion, and large cell undifferentiated histology.7
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


