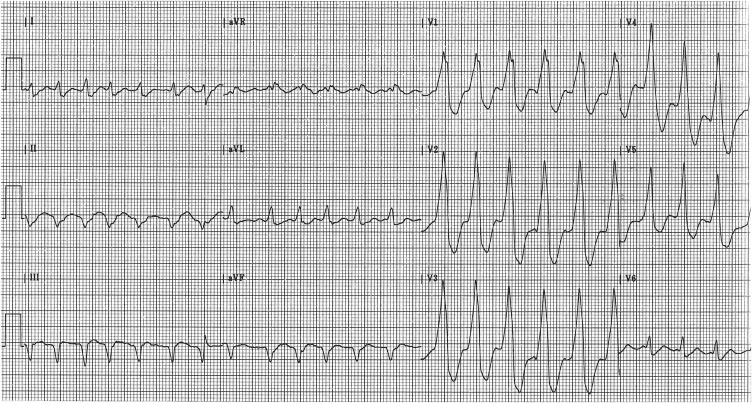
In a woman with rheumatic heart disease, atrial flutter with a rapid ventricular response, and congestive heart failure, treatment with digoxin slows conduction in the atrioventricular node and thus allows atrioventricular conduction to occur by way of a previously unrecognized accessory pathway.
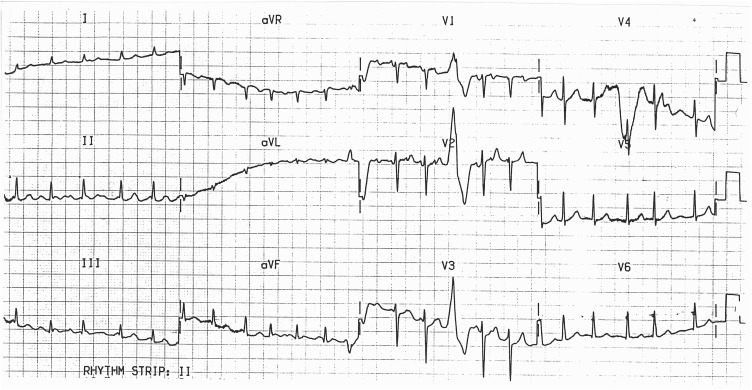
A 53-year-old woman with a history of acute rheumatic fever as a child first presented to the clinic with an irregular narrow-QRS tachycardia ( Figure 1 ). Large left and right ventricular impulses were noted on palpation, and there was a prominent mitral regurgitation murmur. Distended neck veins, peripheral edema, and pulmonary crackles indicated congestive heart failure. She refused hospitalization and was treated with digoxin and a diuretic. When she returned for follow-up 3 days later, her electrocardiogram (ECG) had changed ( Figure 2 ).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


