TABLE 29.1. Biology of myocardial protection | ||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||
between species and is thought to be due to upregulation of 5′-adenosine monophosphate-activated protein kinase (9). During this period of development, the neonatal myocardium shows a progressive decline in glucose uptake which can be stimulated by insulin, that is, insulin resistance and a much greater capacity to store glycogen (10). The greater ability of the immature myocardium to utilize anaerobic glycolysis may partially account for the greater tolerance to ischemia. Laboratory and clinical studies in adults have found that enhanced glucose uptake and oxidation is associated with enhanced functional myocardial recovery, despite normalization of fatty acid oxidation (6).
TABLE 29.2. Physiologic differences between pediatric and adult myocardium and the potential impact of these differences on ischemia tolerance of the pediatric heart | ||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||
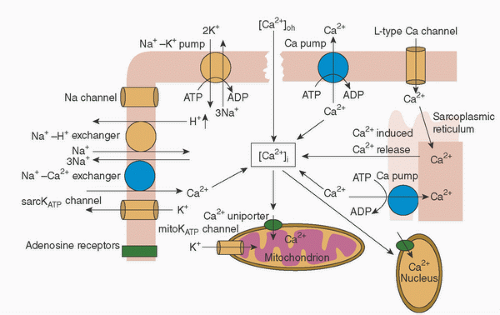 FIGURE 29.1. Sources of calcium regulation. Calcium entry via the L-type Ca2+ channel causes Ca2+ release from the sarcoplasmic reticulum (SR) via the ryanodine receptor (Ca-induced Ca release) and activation of contraction. Calcium is pumped back into the SR by SR Ca2+-ATPase and extruded from the cell by activating the Na+-Ca2+-exchanger to allow relaxation. Calcium can also enter mitochondria via a Ca2+ uniporter. (Reprinted from Levitsky S, McCully JD. Myocardial protection. In: Sellke FW, del Nido PJ, Swanson SJ, eds. Sabiston & Spencer surgery of the chest. 8th ed. Philadelphia, PA: Saunders Elsevier, 2010:977-998, Figure 63-4 (p. 980), with permission.) |
tissue per minute) averaged 6.7 mL in the working state (adult 8 mL), 3.2 mL in the empty beating state (adult 5.6 mL), 1.3 mL in the potassium-arrested heart at 37°C (adult 1.1 mL), 0.37 mL in the hypothermic (15°C) heart, and 0.32 mL in the hypothermic (15°C) potassium-arrested heart (43,44).
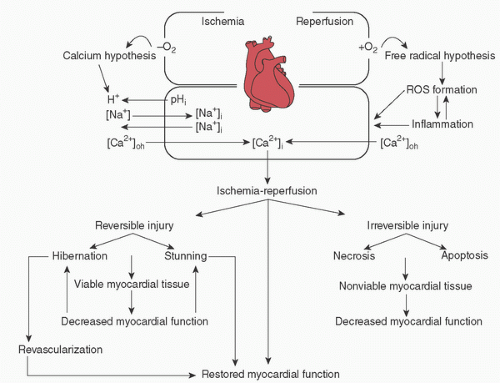 FIGURE 29.2. Mechanisms of ischemia-reperfusion injury. Putative mechanisms of the calcium and free-radical hypotheses and inflammation in the generation of ischemia-reperfusion injury. ROS, reactive oxygen species. (Reprinted from Levitsky S, McCully JD. Myocardial protection. In: Sellke FW, del Nido PJ, Swanson SJ, eds. Sabiston & Spencer surgery of the chest. 8th ed. Philadelphia, PA: Saunders Elsevier, 2010:977-998, Figure 63-3 (p. 980), with permission.) |
(and pulmonary) function as a result of ischemia-reperfusion injury and the associated endothelial dysfunction (49). In neonatal lambs, the addition of L-arginine (NO precursor) or nitroglycerine (NO donor) during reperfusion resulted in significantly higher preload recruitable stroke work and cardiac index (50). A clinical practice at Boston Children’s Hospital is to start a nitroglycerine infusion (1 µg/kg/min) 5 to 10 minutes before removal of the aortic cross-clamp and continue it until the end of rewarming.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


