TABLE 76.1 Histologic Features of Mucinous Adenocarcinomas of the Lung | ||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
such as napsin-A and surfactant proteins (such as SP1) are negative as well.1 Expression of MUC5A5 (secreted tracheobronchial mucin) is present, and MUC2 (secreted intestinal mucin) is absent.4 Mucinous adenocarcinoma in situ is negative for CDX2.1
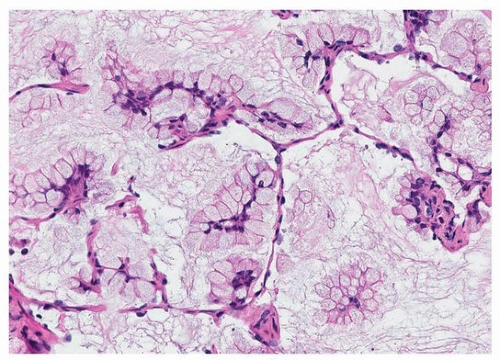 FIGURE 76.1 ▲ Mucinous adenocarcinoma in situ. The alveolar septa are typically thin and normal in appearance. |
 FIGURE 76.2 ▲ Mucinous adenocarcinoma in situ, columnar cells. The lining cells are often columnar, with pseudostratified parallel nuclei at the base. A. Routine stain showing apical mucin vacuoles and intra-alveolar mucin. B. A periodic acid-Schiff stain demonstrates diffuse cytoplasmic mucin, with apparent basal sparing because of the nuclei. |
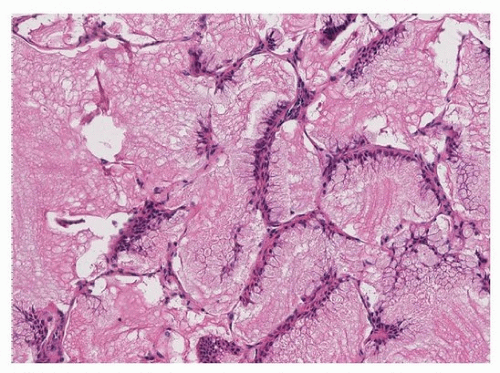 FIGURE 76.3 ▲ Mucinous adenocarcinoma in situ, goblet cell predominance. The lepidic component may have a predominance of goblet cells, with flattened basal nuclei. The tumor cell apices seem to be extruding mucin into the alveolar spaces. |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


