A total cavopulmonary connection (Fontan surgery) is rarely performed in a child with trisomy 21 (Down syndrome) for a univentricular heart, and the outcomes after surgery are not well defined, but the incidence of mortality has been reported to be higher. To determine the mortality rate and contributing factors after Fontan surgery in children with Down syndrome, mortality data after Fontan surgery from the Pediatric Cardiac Care Consortium Registry were evaluated. Among Fontan procedures (n = 2,853), all patients with Down syndrome (n = 17) were selected, of whom 13 had hemodynamic data available. Thirteen children without chromosomal aberrations were then selected as a control group, matched 1 to 1 for gender, age, weight, lesion, and type of Fontan procedure. The following variables were evaluated: pulmonary artery pressure and vascular resistance, weight, hemoglobin, degree of atrioventricular regurgitation, previous Glenn operation, fenestration, and length of stay in the hospital. In children with Down syndrome, mortality after the Glenn operation was 28%. Mortality after the Fontan operation was increased significantly (p = 0.001) in children with Down syndrome (35%) compared with those without Down syndrome (10%). Between patients with Down syndrome and controls, there were no significant differences in the perioperative parameters evaluated. Almost all mortality was in the early postoperative period in children with Down syndrome. The relative risk ratio of mortality was 2.5 (95% confidence interval 0.63 to 10). In conclusion, Down syndrome was found to be an independent parameter associated with a significantly higher risk for mortality in the early postoperative period after Fontan surgery.
Cavopulmonary shunts (Glenn and Fontan surgeries) are among a number of surgical procedures that children with univentricular hearts must undergo to route the systemic venous return into the pulmonary circulation. We hypothesized that children with trisomy 21 (Down syndrome) would have higher pulmonary artery pressure (PAP) compared with those without Down syndrome and would hence have a greater risk for mortality after total cavopulmonary connection (Fontan) surgery. The aims of this study were (1) to determine mortality after Glenn and Fontan procedures and compare the incidence between children with and those without Down syndrome and (2) to determine if the pre-Fontan PAPs obtained by catheterization were higher in children with compared with those without Down syndrome. We accessed data from the Pediatric Cardiac Care Consortium (PCCC) Registry, which collects data from 27 centers in the United States and 4 centers internationally.
Methods
The study was a case-control study using a historical cohort. The PCCC Registry data were collected from 1982 onward, representing an experience of >20 years. The Human Subjects Committee of the University of Minnesota approved the use of deidentified PCCC Registry data for the study. The study population included all children with cardiac malformation who underwent cardiac catheterization or cardiac operations or who died from cardiac conditions, either early or late. For these patients, we had available a computerized database as well as charts with their intake demographic data sheets, echocardiograms, catheterization data, surgical data, and autopsy or death reports. These reports were gathered retrospectively (i.e., the reports were sent in after the procedures were performed or death occurred). Mortality was defined as early mortality when death occurred <30 days after surgery and late when it occurred >30 days after surgery.
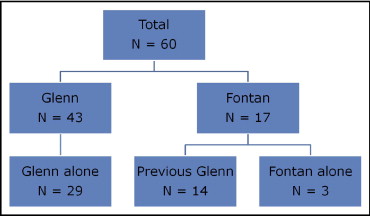
In the PCCC Registry data, there were 4,477 children with Down syndrome who underwent surgical procedures. Sixty cavopulmonary shunts were done in children with trisomy 21, of which 43 were Glenn operations and 17 were Fontan operations ( Figure 1 ). Of the Fontan operations, 3 were Fontan operations alone and 14 were Glenn operations followed by Fontan operations In the database, there were 29 children who underwent Glenn operations alone. We studied the children who underwent Fontan operations (n = 17). Complete hemodynamic data were not available for 4 of these 17 patients (3 unbalanced complete atrioventricular canal and 1 tricuspid atresia); hence, the study group included the remaining 13 patients for whom data were available ( Figure 2 ).
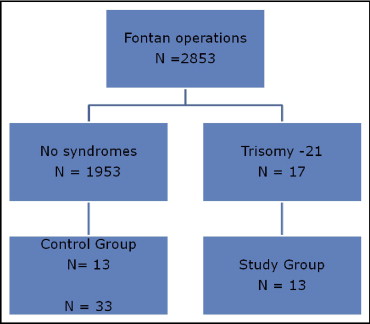
In the PCCC Registry, there were total of 2,853 Fontan operations; these included the first Fontan operation for each patient and also the revision of Fontan ( Figure 2 ). From this population, we selected all children who had no syndromes except for heterotaxia syndrome (n = 1,953). A control group (n = 13) was then selected from this group, matched 1 to 1 for gender, age at Fontan surgery, weight at Fontan surgery, lesion, and types of Glenn and Fontan operations. We evaluated the following preoperative parameters from the PCCC Registry data: age at Fontan operation, gender, weight, hemoglobin, oxygen saturation, mean PAP, pulmonary vascular resistance, degree of atrioventricular valve regurgitation, and previous Glenn operation. We also evaluated other parameters, such as types of Glenn and Fontan operations, fenestration of Fontan baffle, and length of stay in the hospital after Fontan surgery.
Data are expressed as means or percentages as appropriate. We performed Student’s t tests for continuous variables and chi-square or Fisher’s exact tests for dichotomous variables to compare clinical parameters between children with and those without Down syndrome. We conducted paired Student’s t tests for continuous variables and McNemar’s exact tests for dichotomous variables and exact tests of marginal homogeneity for categorical variables to compare the perioperative parameters between the 2 groups for 1:1 matched data. The individual parameters were compared univariately between patients and controls at the local 5% level of significance. Relative risk was calculated by comparing the risk or the ratio of the probability of mortality occurring after Fontan surgery in children with versus those without Down syndrome.
Results
In the entire population of children who underwent Fontan operations (n = 2,853), there was a total of 313 deaths (11%). The overall mortality after Glenn operations in children without Down syndrome was 9%, whereas in those with Down syndrome, it was 28%. Mortality after Fontan surgery ( Table 1 ) was higher in children with versus those without Down syndrome, but there were no significant differences in any of the perioperative criteria evaluated between the 2 groups other than lower weight in children with Down syndrome ( Table 2 ). Most patients with Down syndrome who underwent Fontan operations had unbalanced complete atrioventricular canal defects ( Table 3 ), and none had documented decreased single ventricular systolic function before surgery. The relative risk for mortality after Fontan surgery was calculated at 2.5 for children with Down syndrome (95% confidence interval 0.63 to 10).
| Fontan (n = 2,853) | Fontan and No Syndromes (n = 1,953) | Fontan in Down Syndrome (n = 17) | Fontan in uCAVC and No Syndromes (n = 194) | |
|---|---|---|---|---|
| Deaths | 313 (11%) | 204 (10%) | 6 (35%) | 32 (17%) |
| Variable | Down Syndrome (n = 17) | No Down Syndrome (n = 1,970) | p Value |
|---|---|---|---|
| Age at Fontan surgery (years) | 4.99 ± 4.27 | 6.79 ± 6.43 | 0.25 |
| Weight (kg) | 16.5 ± 9.2 | 21.5 ± 15.2 | 0.04 |
| Hemoglobin (g/dl) | 15.2 ± 2.7 | 15.9 ± 2.7 | 0.24 |
| Length of stay (days) | 21.9 ± 19.7 | 17.95 ± 17.1 | 0.35 |
| Deaths, early | 5 (29%) | 195 (10%) | 0.008 |
| Deaths, late | 1 (6%) | 23 (1%) | 0.18 |
| Age at death (years) | 2.91 ± 1.48 | 7.39 ± 7.41 | <0.0001 |
| Patient | Diagnosis | Glenn Surgery | AVVR Grade | Age (years) | Gender | Weight (kg) | Hemoglobin (g/dl) | S p O 2 (%) | Mean PAP (mm Hg) | PVR (U · m 2 ) | Fontan Surgery | F/NF | LOS (days) | Outcome |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | AVC, HPRV | None ⁎ | 2 | 5 | M | 17.1 | 21.7 | 63 | 18 | 4.3 | MODF | NF | 5 | Dead |
| 2 | AVC, HPRV | None ⁎ | 2 | 5 | M | 18.3 | 18.2 | 82 | 16 | 2.1 | MODF | NF | 76 | Alive |
| 3 | AVC, HPRV | BDG | 1 | 6 | M | 13 | 14 | 88 | 17 | 2.5 | MODF | F | 23 | Alive |
| 4 | AVC, HPRV | BDG | 0 | 3 | F | 15.7 | 12.9 | 93 | 17 | 2.5 | Extracardiac | NF | 7 | Alive |
| 5 | AVC, HPRV | Classic Glenn | 0 | 18 | M | 43.6 | 11.9 | 85 | 20 | 3.9 | MODF | F | 30 | Alive |
| 6 | AVC, HPRV | Hemi-Fontan | 3 | 1.5 | F | 9.3 | 17.1 | 77 | 15 | 2.83 | MODF | F | 22 | Dead |
| 7 | AVC, HPRV | BDG | 2 | 2.5 | M | 10.7 | 17.5 | 85 | 15 | 3.4 | MODF | NF | 5 | Alive |
| 8 | AVC, HPRV | BDG | 1 | 2.5 | F | 10 | 14.5 | 84 | 6 | 3.7 | MODF | F | 37 | Dead |
| 9 | AVC, HPRV, PS | BDG | 0 | 0.5 | F | 6.4 | 19.6 | 77 | 10 | 3.5 | MODF | NF | 8 | Alive |
| 10 | AVC, HPRV, TOF | BDG | 2 | 3.5 | M | 16.5 | 13 | 85 | 15 | 2.9 | Extracardiac | NF | 23 | Dead |
| 11 | PA, IVS, HPRV | BDG | 0 | 2.7 | F | 10.5 | 13.8 | 86 | 7 | 0.83 | MODF | NF | 10 | Alive |
| 12 | AVC, HPLV, PS, HET | None ⁎ | 1 | 10 | M | 30 | 18.9 | 83 | 16 | MODF | F | 17 | Alive | |
| 13 | AVC, HPLV | BDG | 0 | 2.5 | F | 9.2 | 14 | 75 | 8 | 3.3 | Classic (atriopulmonary) Fontan | NF | 8 | Dead |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


