By far, the most common cause of mitral stenosis is rheumatic fever (1,2). This inflammation-induced valvular disease results in fusion of the leaflet commissures as well as thickening, fusion, and shortening of the chordae tendineae. Interestingly, only about half of affected patients actually report a clinical history of rheumatic fever (3). Another cause of mitral stenosis is the functional stenosis caused by mitral annular calcification, which can lead to restricted leaflet motion. This type of mitral stenosis is rarely severe and is most commonly found in the elderly. Other causes of mitral stenosis include congenital mitral valve lesions that are almost always diagnosed in infancy or early childhood (4), and systemic disorders such as systemic lupus erythematosus, rheumatoid arthritis, and amyloidosis. Although extremely rare, in patients with a history of methysergide exposure, mitral stenosis has been reported to develop (5).
PRESENTING SIGNS AND SYMPTOMS
The most common symptoms in patients with mitral stenosis are dyspnea on exertion and decreased exercise tolerance. Because either of these symptoms may be present in an array of systemic disorders, mitral stenosis is sometimes an elusive diagnosis. In previously undiagnosed advanced cases, a patient may be first seen with acute left-sided heart failure. Hemoptysis has been reported as one of the clinical signs of mitral stenosis (6) and may be either an incidental finding or life-threatening and lead to acute cardiopulmonary failure (7). The presence of atrial fibrillation is extremely common with mitral stenosis, and a cardioembolic event may be the presenting sign in some patients (8).
Because this disorder represents a fixed obstruction to flow between the left atrium and the left ventricle, any condition that causes an abrupt and significant increase in a patient’s basal heart rate may induce clinical decompensation. For example, patients with atrial fibrillation who are not taking adequate AV-nodal blocking agents are prone to acute left-sided heart failure should a rapid ventricular rate develop. Respiratory infections, physical or emotional stress, or pregnancy are also physiologic situations that may induce acute cardiopulmonary symptoms in patients with mitral stenosis.
Ten to fifteen percent of patients may have chest pain. Potential etiologies include coronary emboli arising from atrial fibrillation, concomitant coronary atherosclerosis, or right ventricular strain from advanced pulmonary hypertension (6). Rarely, a patient may have hoarseness secondary to left recurrent laryngeal nerve paralysis. Physiologically, this is due to nerve entrapment between the aorta, an enlarged pulmonary artery, and the ligamentum arteriosum, and is referred to as Ortner syndrome (9).
The physical examination of patients with mitral stenosis is characterized by a rumbling diastolic murmur heard best with the bell of the stethoscope placed near the cardiac apex while the patient is in a left lateral recumbent position. An opening snap (OS) may be heard secondary to the abrupt halt in leaflet motion during diastole and is best heard when the leaflets are still pliable. It is helpful to note that the earlier the OS occurs after S2, the more severe the mitral stenosis. Other physical examination findings may include a prominent S1 and rales secondary to pulmonary edema. If secondary pulmonary hypertension has developed, a loud P2, an RV heave, a loud tricuspid regurgitation murmur, or a combination of these may also be appreciated.
HELPFUL TESTS
The electrocardiogram in mitral stenosis will often show signs of left atrial enlargement. In more severe forms of mitral stenosis, evidence of right ventricular hypertrophy, right axis deviation, and right atrial enlargement also may be seen. The chest radiograph may reveal straightening of the left heart border, suggesting left atrial enlargement, and may show evidence of interstitial edema. If significant pulmonary hypertension is present, enlargement of the right heart and pulmonary arteries also may be present. A highly calcified mitral valve annulus may sometimes be seen on the chest radiograph.
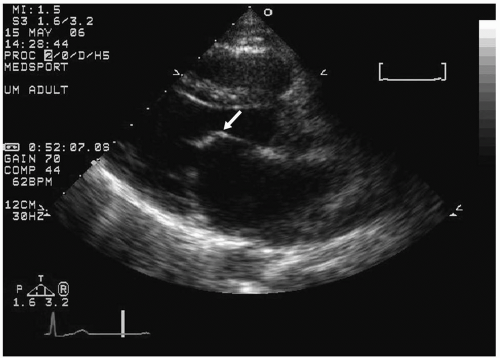
FIGURE 23.1. Two-dimensional echocardiographic image of a patient with rheumatic mitral stenosis. Arrow, Classic diastolic doming, or “hockey-stick” appearance of the anterior mitral valve leaflet.
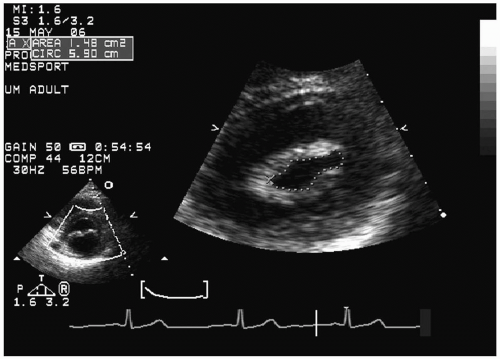
Echocardiography is the mainstay of diagnostic testing in mitral stenosis. Two-dimensional echocardiography allows visualization of the mitral valve anatomy and leaflet motion. Patients with rheumatic mitral stenosis typically have commissural fusion of the leaflets, producing the classic “diastolic doming” or “hockey-stick” appearance of the anterior mitral valve leaflet when viewed in the parasternal long-axis view (Fig. 23.1). The short-axis view of the mitral valve allows direct planimetry of the maximal orifice size during diastole for determination of the mitral valve area (Fig. 23.2) (10).
Doppler examination allows measurement of the mean pressure gradient across the mitral valve (Fig. 23.3)(11), as well as measurement of the right ventricular systolic pressure (RVSP) from the tricuspid regurgitation jet. In the absence of pulmonic stenosis, the RVSP is equal to the pulmonary artery systolic pressure (PASP) and provides a way of assessing pulmonary hypertension. Color Doppler allows assessment of any concomitant mitral regurgitation. The mitral valve area can also be determined from the Doppler spectrum of the mitral inflow by using the pressure half-time method:
FIGURE 23.2. Planimetry of the mitral valve area in a patient with mild-to-moderate mitral stenosis.
FIGURE 23.3. Doppler echocardiography revealing an elevated mean gradient of 29 mm Hg in a patient with severe mitral stenosis.
mitral valve area = 220/P½ time
where P½ time represents the time interval for the mitral valve pressure gradient to decrease by 50% (11,12). This equation is less accurate in the setting of aortic regurgitation, changing HR, or altered atrial or ventricular compliance (13,14,15,16). Other less commonly used methods to determine the mitral valve area include the continuity equation (17) and the PISA (proximal isovelocity surface area) method with angle correction (18).
Grading the severity of mitral stenosis is based on a number of factors, including the mean gradient, the valve area, and the pulmonary artery systolic pressure. The classification of the severity of mitral stenosis is shown in Table 23.1 (19). In patients suspected of having symptoms secondary to mitral stenosis but who have low mitral valve gradients at rest, echocardiography can be performed during leg lifts or supine bicycle exercise to assess exercise-induced increase in the mitral valve mean gradient or right ventricular systolic pressure (20,21).
The degree of mitral stenosis also can be assessed by transesophageal echocardiography (TEE) or cardiac catheterization, although these approaches are usually reserved for patients who do not have an adequate evaluation on transthoracic echocardiography (TTE) or patients who are being considered for percutaneous or surgical intervention. TEE provides superior assessment for thrombus within the left atrium and left atrial appendage, which is crucial to identify before inserting a balloon catheter for valvuloplasty. TEE also provides higher-resolution images of the mitral valve.
TABLE 23.1.Classification of the severity of mitral stenosis in adults
MILD
MODERATE
SEVERE
Mean gradient (mm Hg)
<5
5-10
>10
Pulmonary artery systolic pressure (mm Hg)
<30
30-50
>50
Valve area (cm2)
>1.5
1.0-1.5
<1.0
Valve gradients are flow dependent and, when used as estimates of severity of valve stenosis, should be assessed with knowledge of cardiac output or forward flow across the valve.
Reproduced with permission from: Bonow RO, Carabello BA, Chatterjee K, et al. ACC/AHA 2006 guidelines for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 1998 Guidelines for the Management of Patients with Valvular Heart Disease) developed in collaboration with the Society of Cardiovascular Anesthesiologists endorsed by the Society for Cardiovascular Angiography and Interventions and the Society of Thoracic Surgeons. Circulation 2006;114:e84-e231.
Invasive evaluation of mitral stenosis during cardiac catheterization allows simultaneous measurement of the left ventricular pressure and the pulmonary capillary wedge pressure (as a surrogate of the left atrial pressure). From these measurements, a mean mitral valve pressure gradient can be determined. By measuring flow with the Fick or thermodilution cardiac output, the mitral valve area also can be calculated by using the Gorlin equation. Potential pitfalls include variability in the cardiac output measurement and the use of the PCWP as a surrogate of LA pressure, which may lead to overestimation of the mitral valve gradient (22). In rare cases, a transseptal puncture can be performed to measure the LA pressure directly, if necessary. Cardiac catheterization also allows direct measurement of the right ventricular and pulmonary artery systolic pressures.
Only gold members can continue reading. Log In or Register to continue