(1)
Department of General surgery, Fuwai Hospital, Beijing, China
18.1 General Considerations
Hypoplastic left ventricle, also termed hypoplastic left heart syndrome, is often associated with a variety of deformities, such as AV and aortic arch anomalies. The specimens presented in this chapter are limited to show mitral atresia and mild hypoplastic LV.
18.2 Mitral Atresia
Muscular atresia and membranous atresia are two morphological subtypes of mitral atresia. The former may result from the directional abnormity of the development of the ventricular septum, and the muscular tissue occludes the atrioventricular orifice. The latter may result from the over fusion of the endocardial cushion, which results in the MV leaflets being fused together. Mitral atresia inevitably combines defects of the atrial or ventricular septum, patent ductus arteriosus, and hypoplastic LV.
18.3 Hypoplastic Left Ventricle
The specimens shown in this chapter are mainly those of mild hypoplasia of the LV. The LV is relatively small and thin walled, with mitral or aortic valve malformation. Specimen NO. 1025 (Fig. 18.2) shows dysplasia of the LV, MV, and aorta. It could be referred to as hypoplastic left heart syndrome. The RA and RV may have varying degrees of dilation.
18.4 Specimen Demonstrations
18.4.1 Mitral Atresia Combined with Pulmonary Atresia
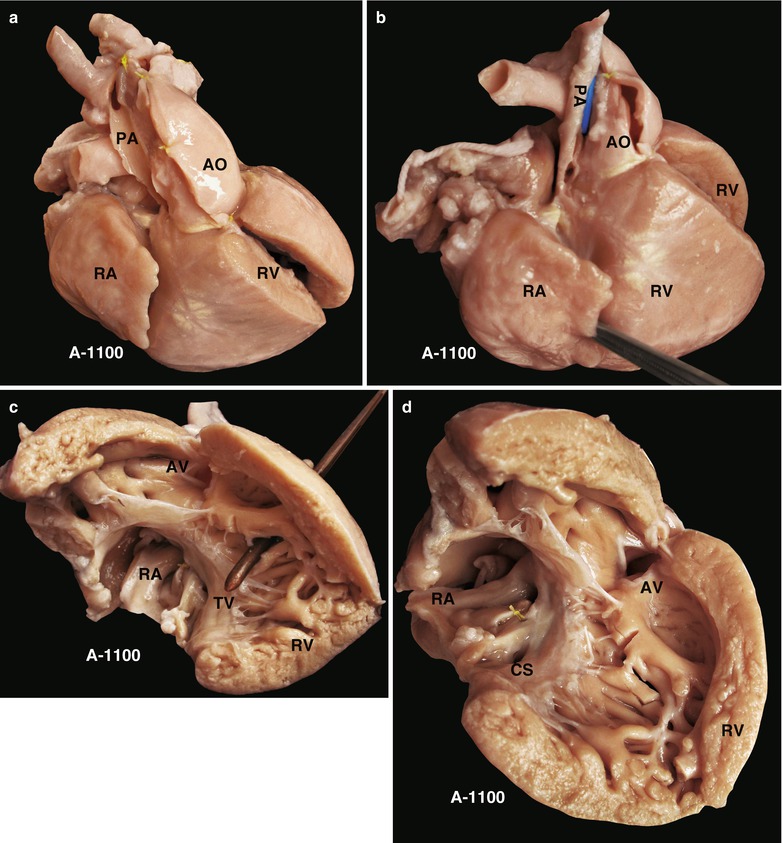
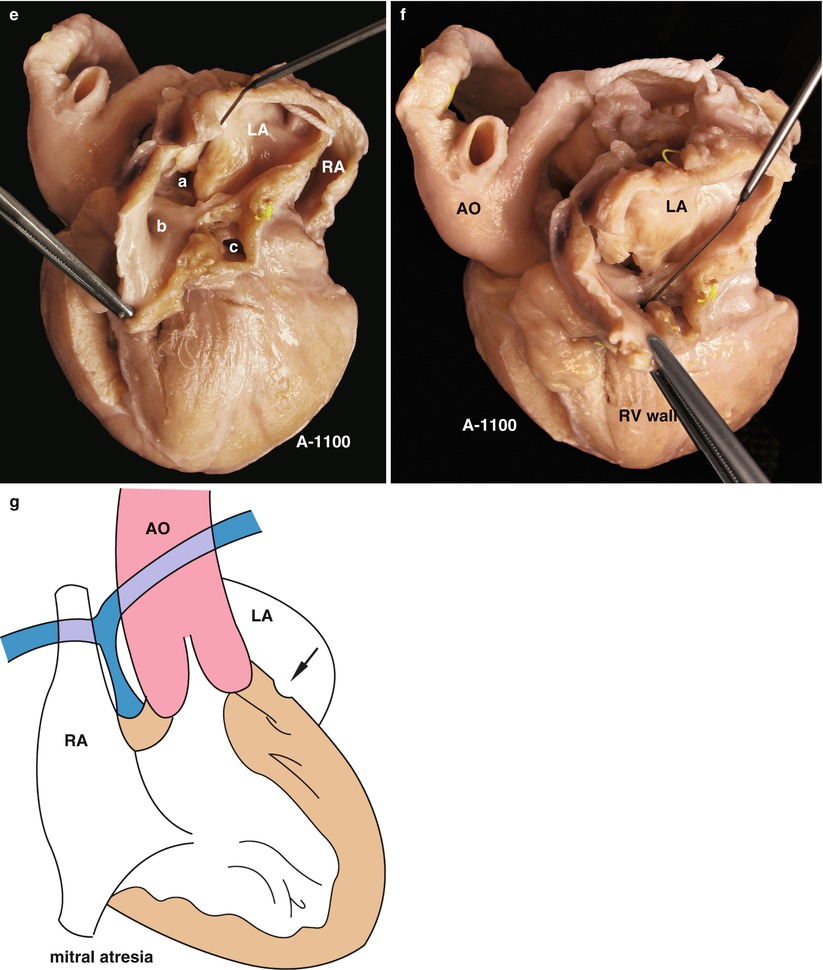
Fig. 18.1
(a) Specimen 1100. The frontal view of mitral atresia combined with pulmonary atresia shows the fine main pulmonary artery at the back of the aorta. (b) Specimen 1100. The blue bougie indicates the fine main pulmonary artery. The blind-end root confirms the pulmonary atresia. RA hypertrophic and dilated right atrium, RV right ventricle, the only ventricular chamber of this specimen. (c) Specimen 1100. Ventricular anterior wall opened to expose the right atrium and outflow tract of the right ventricle. The structure of the atrioventricular valve conforms to the characteristics of the TV. The multiple muscle trabeculae, conical muscle-like structures between the aortic and tricuspid valves, could confirm that the chamber is morphologically the RV. The RVOT links with the AV. The PV does not exist in the chamber. The features confirm that the left side does not have a chamber, which is equivalent to a single ventricle with right ventricular morphology. AV aortic valve, RA right atrium, RV morphological right ventricle, RVOT right ventricular outflow tract, TV tricuspid valve. (d) Specimen 1100. Exposure of the aortic valve orifice and subvalvular myocardial infundibulum. AV aortic valve, CS coronary sinus, RA right atrium, RV right ventricle. (e) Specimen 1100. Exposure of the left atrium without the mitral valve. a, atrial septal defect; b, left atrial appendage; c, rupture of the coronary sinus; LA left atrium, RA right atrium. (f) Specimen 1100. Mitral atresia. No MV is found in the LA. The bougie indicates the residual recess. The ventricular wall under the atrium belongs to the morphological RV (RV wall). AO aorta. (g) Schematic diagram of specimen 1100. The ventricle has structures characteristic of the RV. The RA has inlets of the coronary sinus and the vena cava. These features prove the atrium is in situ solitus. The mitral atresia remains a recess without a LV chamber
< div class='tao-gold-member'>
Only gold members can continue reading. Log In or Register to continue
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


