Mesothelioma
Presentation
A 62-year-old man is admitted to the medical service with complaints of dry cough, chest discomfort, and dyspnea for the past 3 months. The chest discomfort is mildly painful, is localized to the left side of the chest, does not radiate, and involves the left shoulder. The patient reports a fever (oral temperature of 101.5°F) but no night sweats or chills. On physical examination, vital signs are stable, and oxygen saturation is 93%. Examination of the chest reveals dullness and diminished breath sounds on the left side. The patient denies weight loss. Social history reveals a nonsmoking patient who for 24 years worked in dismantling old buildings and construction. You are being consulted after the following chest x-rays and computed tomography (CT) scans are obtained.
▪ Chest X-rays
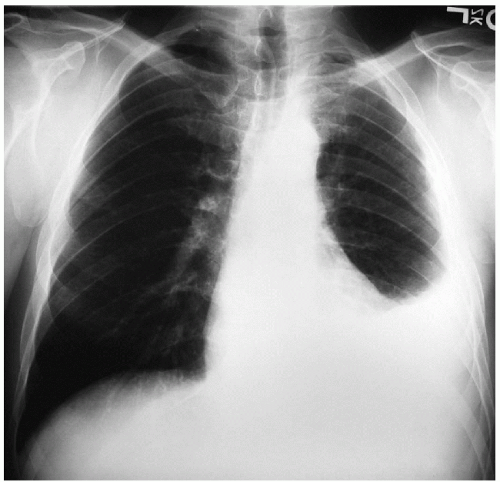 Figure 11-1 |
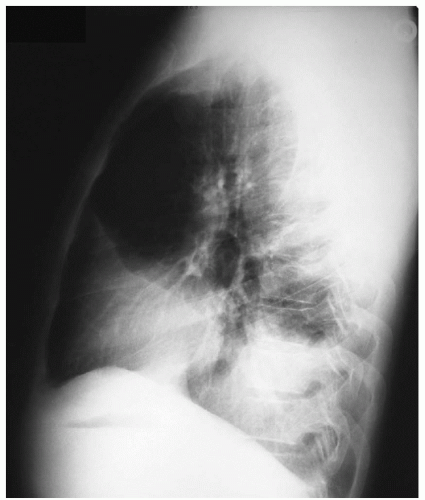 Figure 11-2 |
Chest X-ray Report
The chest x-ray demonstrates a left pleural effusion. There are no lung nodules in both lung fields. The heart is not enlarged.
▪ CT Scans
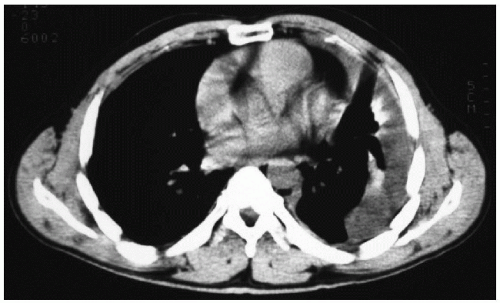 Figure 11-3 |
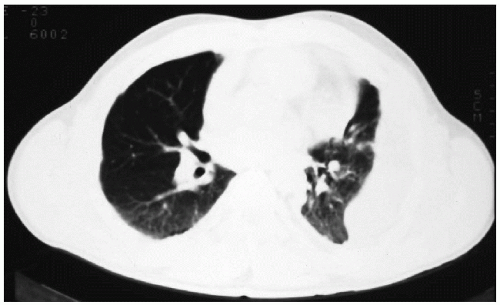 Figure 11-4 |
CT Scan Report
The CT scans demonstrate a loculated effusion encasing the left lung, with a significant volume loss. There is no evidence of lung nodules.
Case Continued
A diagnostic thoracentesis is performed. The fluid is amber and exudative. The glucose level is 60 mg/dL, and the pH is 7.15. Cytologic examination demonstrates mesothelial cells, lymphocytes, and polymorphonuclear leukocytes. Some cells appear suspicious for malignancy. The patient’s symptoms of dyspnea improve minimally.
Discussion
Given the patient’s occupational history and the possibility of exposure to asbestos, mesothelioma should be strongly considered. Adenocarcinoma of the lung with involvement of the pleura is also in the differential diagnosis. Infectious causes are less likely given the clinical presentation of this patient. Thoracentesis demonstrates positive cytology in 30% to 50% of patients with mesothelioma. In comparison, needle pleural biopsy is positive in only 30% of the patients. It is often not feasible to confirm malignancy on cytologic specimens in this setting. Fur thermore, distinguishing between mesothelioma and adenocarcinoma is difficult by light microscopy alone. Early mesotheliomas may not be easily distinguished from benign mesothelial hyperplasia or severe fibrosis because of the cell types found in such tumors. Because the treatment is dependent on a definite diagnosis, a more substantial quantity of a specimen should be obtained
to perform immunohistochemical assays and electron microscopy. Furthermore, diffuse malignant mesothelioma can be histologically confused with metastatic adenocarcinoma or sarcoma. Several histologic stains that enable differentiation of mesothelioma from other diagnoses are available to the pathologist. Adenocarcinomas usually stain with mucicarmine, whereas mesotheliomas do not. Mesotheliomas stain for certain cytokeratins, which may differentiate them from sarcomas, whereas they do not stain for carcinoembryonic antigen (CEA), which is usually seen with adenocarcinoma. Electron microscopy displays the numerous long sinuous microvilli of mesothelioma or the short straight microvilli of an adenocarcinoma as well as the presence of intracellular desmosomes, junctional complexes, and characteristic microvilli. Proper preparation of the specimen is essential when mesothelioma is suspected. Part of the specimen is fixed in neutral buffered formalin, and the rest is fixed with glutaraldehyde preparation for electron microscopy examination.
to perform immunohistochemical assays and electron microscopy. Furthermore, diffuse malignant mesothelioma can be histologically confused with metastatic adenocarcinoma or sarcoma. Several histologic stains that enable differentiation of mesothelioma from other diagnoses are available to the pathologist. Adenocarcinomas usually stain with mucicarmine, whereas mesotheliomas do not. Mesotheliomas stain for certain cytokeratins, which may differentiate them from sarcomas, whereas they do not stain for carcinoembryonic antigen (CEA), which is usually seen with adenocarcinoma. Electron microscopy displays the numerous long sinuous microvilli of mesothelioma or the short straight microvilli of an adenocarcinoma as well as the presence of intracellular desmosomes, junctional complexes, and characteristic microvilli. Proper preparation of the specimen is essential when mesothelioma is suspected. Part of the specimen is fixed in neutral buffered formalin, and the rest is fixed with glutaraldehyde preparation for electron microscopy examination.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


