Systolic anterior motion of the mitral valve (SAM) occurs intraoperatively after mitral valve repair (MVRr) in up to 14% of cases and typically resolves in the operating room with conservative measures. Less commonly SAM may also occur in the early or late postoperative period. The clinical course and optimal management of such cases is poorly defined, but reoperation is common. We describe our experience using disopyramide to successfully treat postoperative SAM refractory to beta blockade. Seven patients were retrospectively identified with mitral valve prolapse who underwent MVRr from 2003 to 2015 and were found during follow-up to have severe SAM with a left ventricular outflow tract (LVOT) gradient not observed intraoperatively. All 7 patients were successfully managed medically. In 5 cases, SAM persisted even after maximization of beta blockade, and the addition of disopyramide led to significant improvement or resolution of SAM, the LVOT gradient, and mitral regurgitation. The postoperative LVOT gradient initially exceeded 30 mm Hg in 6 of 7 patients. In 2 patients, the LVOT gradient exceeded 100 mm Hg, and both were managed medically with disopyramide with complete resolution of SAM. In conclusion, SAM after MVRr typically follows a benign clinical course and can be managed medically in most cases. When an initial treatment strategy of beta blockade is insufficient, the addition of disopyramide can effectively alleviate and terminate this condition and should be considered before reoperation.
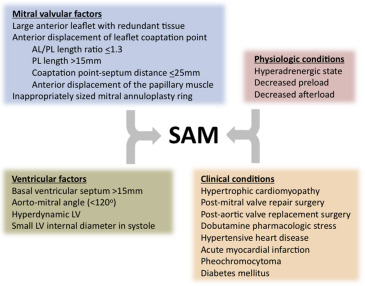
Systolic anterior motion of the mitral valve (SAM) is a well-described phenomenon associated with mitral regurgitation (MR) and usually a left ventricular outflow tract (LVOT) peak systolic gradient. This gradient, SAM, and MR are dynamic and highly sensitive to the size and inotropic state of the left ventricle. SAM and LVOT gradients may occur in a variety of conditions and physiologic states ( Figure 1 ), including after mitral valve repair (MVRr). The incidence of SAM after MVRr with an annuloplasty ring has been reported to be as high as 14% in the immediate postrepair period in the operating room, with more recent series reporting rates of 6% to 8%. In most cases, up to 85% in some series, medical management in the operating room with volume loading and beta blockade reduces or eliminates the SAM, MR, and LVOT gradient. Much less commonly, SAM after MVRr may recur or newly occur in the early or late postoperative setting as ventricular contractility and loading conditions evolve. The clinical course and optimal management of such cases is less clear. Medical management has been reported to be successful in small numbers of patients with β blockers, but repeat intervention is common. This report describes a single-center experience using disopyramide to successfully treat postoperative SAM refractory to β blockers alone.
Methods
Seven patients were retrospectively identified with a history of mitral valve prolapse, defined as type II by the Carpentier classification, who underwent MVRr between 2003 and March 2015 at Cedars-Sinai Medical Center (Los Angeles, California) and were found at any time during the postoperative period to have severe SAM not observed intraoperatively. In 5 cases, partial or complete posterior leaflet resection was performed with placement of an incomplete mitral annuloplasty ring—4 with an ATS band (ATS Medical, Inc., Minneapolis, Minnesota) and one with a CG Future band (Medtronic, Inc, Minneapolis, Minnesota). In one patient, posterior leaflet resection was not performed, and a Carpentier-Edwards Physio ring (Edwards Lifesciences Corp, Irvine, California) was placed. Surgical details were not available in one patient. Severe SAM was identified by 2-dimensional echocardiography and defined as any portion of the mitral valve that protruded into the LVOT during systole and was associated with either an LVOT gradient of at least 30 mm Hg or greater than mild MR. Patients were followed until February 2016 by chart review for available information pertaining to symptom status, clinical outcome, medication management, and follow-up echocardiograms. No patients underwent an invasive assessment of the LVOT gradient.
Results
As demonstrated in Table 1 , 7 patients were identified with severe SAM with the presence of an LVOT gradient that was not observed intraoperatively, but first noted postoperatively. SAM was noted within the first 3 days postoperatively in 3 of 7 patients, by the end of 10 days postoperatively in 2 other patients, and beyond 20 months postoperatively in 2 patients. The LVOT gradient exceeded 30 mm Hg in all patients at rest or with the Valsalva maneuver and exceeded 50 mm Hg in 5 patients. Two patients had LVOT gradients exceeding 100 mm Hg at rest, and a third developed a gradient >100 mm Hg (184 mm Hg) after initial therapy.
| Patient | Age (Years) / Gender | Surgical details | First Detection of SAM | Interim Medical Therapy | Interim Follow-up | Interim Medical Therapy | Final Follow-up | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Pre-op Mitral Pathology | MVRr Technique, Size (mm) | Posterior Leaflet Resection | Time of Follow-up (Post-op Days) | MR Grade ∗ | Resting (Provoked) LVOT Gradient (mmHg) | B | D | Time of Follow-up (Post-op Days) | SAM | MR Grade ∗ | Resting LVOT Gradient (mmHg) | B | D | Time of Follow-up (Post-op Days) | SAM | MR Grade ∗ | Resting LVOT Gradient (mmHg) | ||
| 1 | 54M | Bileaflet prolapse | ATS band, 39 | + | 2 | 3+ | 24 (33) | + | 0 | 23 | 0 | 1+ | 0 | + | 0 | 760 | 0 | 0 | 0 |
| 2 | 49M | Flail P1 | ATS band, 35 | + | 3 | 0 | 58 (96) | + | 0 | 4 | + | 2+ | 65 | + | + | 17 | 0 | 0 | 0 |
| 3 | 65F | Flail P2 | ATS band, 35 | + | 3 | 4+ | 26 | + | 0 | 6 | + | 2+ | 46 | + | + | 20 | 0 | 0 | 0 |
| 4 | 73M | – | – | – | 7 | 1+ | 52 | 0 † | 0 | 8.8 years | + | 1+ | 184 | 0 ‡ | 0 | 9.9 years | 0 | 0 | 0 |
| 5 | 60M | Bileaflet prolapse | Carpentier-Edwards Physio ring, 28 | 0 | 10 | 4+ | 129 | + | 0 | 13 | + | 4+ | 87 | + | + | 26 | + | 1+ | 42 |
| 6 | 59M | Flail P2 | ATS band, 35 | + | 649 | 3+ | 50 | + | 0 | 8.7 years | + | 4+ | 64 | + | + | 8.8 years | 0 | 0 | 0 |
| 7 | 63M | Flail P2 | CG Future band, 32 | + | 7.5 years | 2+ | 110 | + | 0 | 9.8 years | + | 3+ | 55 | + | + | 9.9 years | + | 3+ | 26 |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


