Cardiovascular magnetic resonance (CMR) is a high spatial resolution, 3-dimensional tomographic imaging technique which may identify regions of massive left ventricular hypertrophy (particularly when confined to the anterolateral free wall) in which the extent of wall thickness is underestimated with traditional 2-dimensional echocardiography in patients with hypertrophic cardiomyopathy (HC). This observation may have potential implications on management strategies as extreme left ventricular hypertrophy is a primary risk factor for sudden death in HC and therefore supports an expanding role for CMR in the evaluation of HC patients.
Case Descriptions
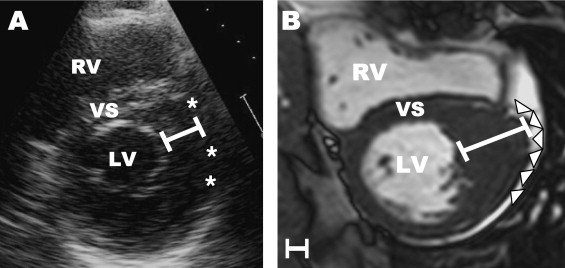
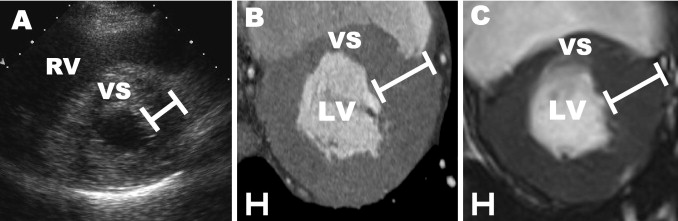
The cardiovascular magnetic resonance (CMR) images presented herein ( Figures 1 to 3 ) expand the role of advanced imaging techniques for hypertrophic cardiomyopathy (HC). CMR (and computed tomography) identified massive degrees of left ventricular (LV) wall thickening (≥30 mm), confined to the anterolateral free wall and substantially underestimated in magnitude by cross-sectional 2-dimensional echocardiography.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


