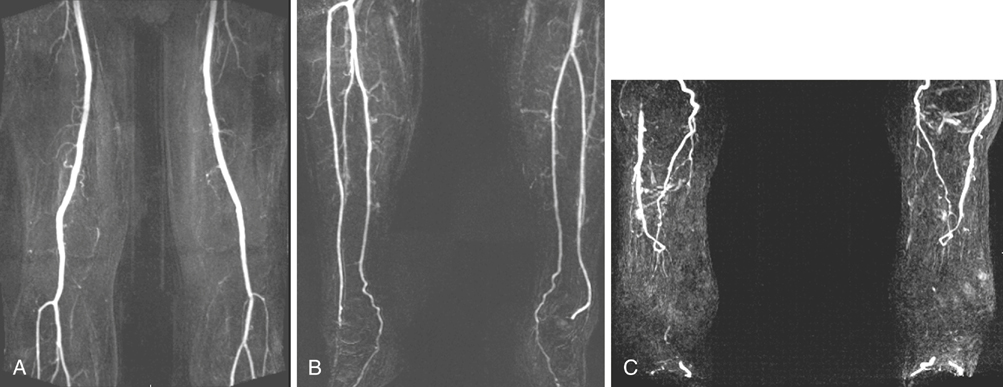
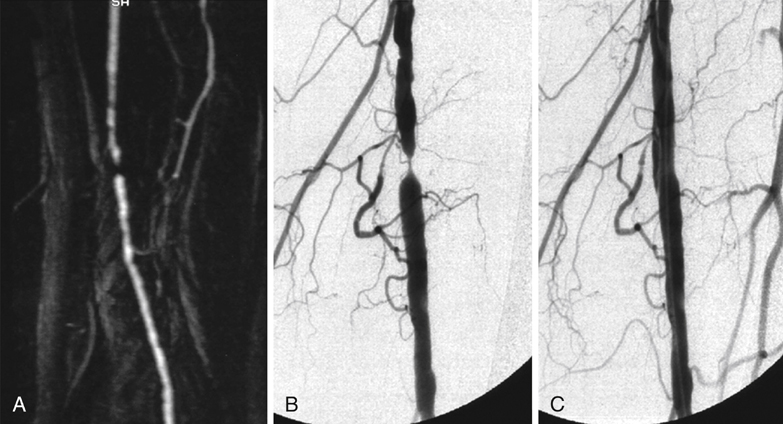
Technological advances have enabled MRA to acquire higher-resolution images in less time. Images may be obtained by noncontrast or contrast-enhanced methods. Time-of-flight (TOF) noncontrast imaging is based on signal differences between saturated and unsaturated protons in blood. This technique has limited use in the era of contrast-enhanced MRA, and it is employed when contrast is contraindicated. Contrast-enhanced MRA most often uses gadolinium, which is an element whose properties shorten the T1 relaxation, causing blood to be more visible than the surrounding tissues (Figure 1). It is designed to produce an effect on the protons in the surrounding water. Thus, minute amounts of MRA contrast may be detected by its effect on multiple water molecules, whereas an equivalent dose of iodinated contrast is not detectable directly by conventional arteriography or computed tomography angiography (CTA). Contrast agents with different properties are under investigation to determine if they improve image quality, sensitivity, or specificity of MRA. In comparison to selective DSA, contrast-enhanced MRA performs equally well in high-flow arterial segments (Figure 2). The differences become more apparent in low-flow regions, with MRA visualizing more segments in the tibial artery that were considered occluded by DSA evaluation (100% sensitivity and specificity). Overall, contast-enhanced MRA was ascertained to be comparable to DSA, with 100% and 98% accuracy, respectively. A common finding noted in the literature is that DSA or conventional arteriography overestimates occlusions, likely affecting surgical interventions and outcomes. MRA reliably detects patent runoff vessels that are occult to conventional arteriography, leading to a higher limb-salvage rate by facilitating reconstructive surgical options.
Magnetic Resonance Arteriography for Assessment of Infrainguinal Occlusive Disease
Fundamental Principles of Magnetic Resonance Arteriography
Clinical Experience with Magnetic Resonance Arteriography
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Thoracic Key
Fastest Thoracic Insight Engine