Figure 21.1
Intralobar sequestration
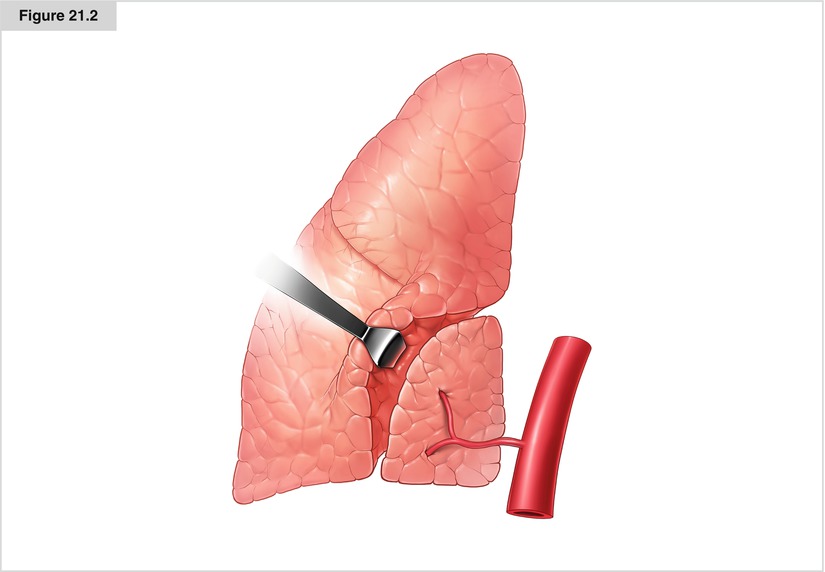
Figure 21.2
Extralobar sequestration
Clinical Presentation
The clinical presentation depends mainly on the type of sequestration. Extralobar sequestration may be detected antenatally by ultrasound. Otherwise, the malformation becomes clinically apparent through respiratory symptoms induced by concomitant anomalies or severe arteriovenous shunting. Male children are more affected, and the left lower part of the thorax is mostly involved; the diagnosis is made within the first year of life. Intralobar sequestration is not detected until recurrent bronchopulmonary infection leads to radiologic examination; therefore, most patients present in adulthood. Segmental infiltration in the dorsal part of the lower lobes in otherwise healthy patients should lead one to suspect this malformation (Corbett and Humphrey 2004). MRI with visualization of the aberrant vessels is used to confirm the radiographic and ultrasound diagnosis (Fig. 21.3).
Surgical Treatment
In every case, the thoracic surgeon must be aware of the anatomic details of the aberrant vessels. In extralobar sequestration, resection of the supplementary lung is combined with correction of other anomalies, such as diaphragmatic hernia, other lung malformations, and cardiac or vascular abnormalities. Intralobar sequestration requires an atypical segmental resection or lobectomy, depending on the extent of the sequestration in the lobe (Fig. 21.4).

Figure 21.3




Frontal magnetic resonance image of the thorax of a 5-month-old boy with hemoptysis and intralobar sequestration. The important systemic blood flow is drained by the lower pulmonary vein. Contrast-enhanced radiologic examinations has to be checked for atypical vessels arising from the descending aorta in all cases of infiltration of the lower lobes, especially in cases with recurrent disease. The anatomy of the pathologic vessel has to be realized to plan the surgical procedure. Since the blood is drained by the veins of the lower lobe, the sublobar resection of the sequestration should respect the venous flow of the healthy lung to avoid lung infarction
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
