Origin of the different bronchopulmonary malformations
Epidemiology
It has been difficult to estimate the precise incidence of lung malformations, and because they are asymptomatic lesions, many authors consider that their frequency may be undervalued. In 2008, the European Record for the vigilance of congenital malformations (Eurocat) estimated an incidence rate of congenital chest malformations at 3.5 per 10,000 live births. The estimated incidence of cystic adenomatoid malformation was 0.7 per 10,000 live births.
Congenital Malformations of the Lung
Cystic Adenomatoid Malformation
The first case of cystic adenomatoid malformation described was published by Ch’in and Tang in 1947. In 1975, Garret conducted the first antenatal diagnostic report of a cystic adenomatoid malformation using echography. Today, almost 90% of these malformations are diagnosed before birth, and correspond to small lesions that are almost always asymptomatic, at least during the neonatal period.
These malformations are cystic lesions that are circumscribed to a segment or lung lobe in more than 95% of the cases, and any lobe may be compromised. Bilateral lesions are rare (<3%) and have a poor prognosis. Histology reveals a proliferation of terminal bronchioles, which form communicated cysts covered in respiratory epithelium with different degrees of differentiation, as well as a reduction in the number of alveoli. There is no cartilage and there is an increase of the elastic fibers. The exact cause of cystic adenomatoid malformation is unknown, and there are arguments to sustain that its different types can originate in different stages of the lung development process. Bronchiolar types (type 1, 2, and 3) may develop during the pseudo-glandular phase, while those of the acinar-alveolar type (type 4) may be the consequence of a late injury in the saccular stage. It has been proven that in cystic adenomatoid malformations there is an increase in the proliferation and a reduction of apoptosis. All these details give strength to the hypothesis of a localized interruption during lung maturation.
Classification of congenital lung malformations in the lung airway
Incidence | Size of cysts | Histology | Notes | |
|---|---|---|---|---|
0 | Infrequent | Complete failure of development after pseudo-glandular phase | Congenital acinar dysplasia (lethal) | |
1 | Frequent 50% | >2 cm, may be multiple | Dilated alveolar structure, with scarce to minimum adenomatoid component. Ciliated pseudostratified columnar epithelium, with interposition of mucosal cells | |
2 | Frequent 40%–45% | Multiple cysts, small, “sponge” | Dilation of structures with bronchial appearance, with interposition of the alveolar parenchyma. Occasional presence of striated muscle. | Associated with genitourinary and gastrointestinal malformations |
3 | Infrequent 5% | Solid (cysts <3 mm) | Bronchiolar structures separated by small air spaces covered by the cuboidal epithelium, similar to late fetal lung | |
4 | Very infrequent | Large cysts | Peripheral cysts with alveolar or bronchial epithelium on elastic mesenchymal tissue | Related to type pleuropulmonary blastoma |
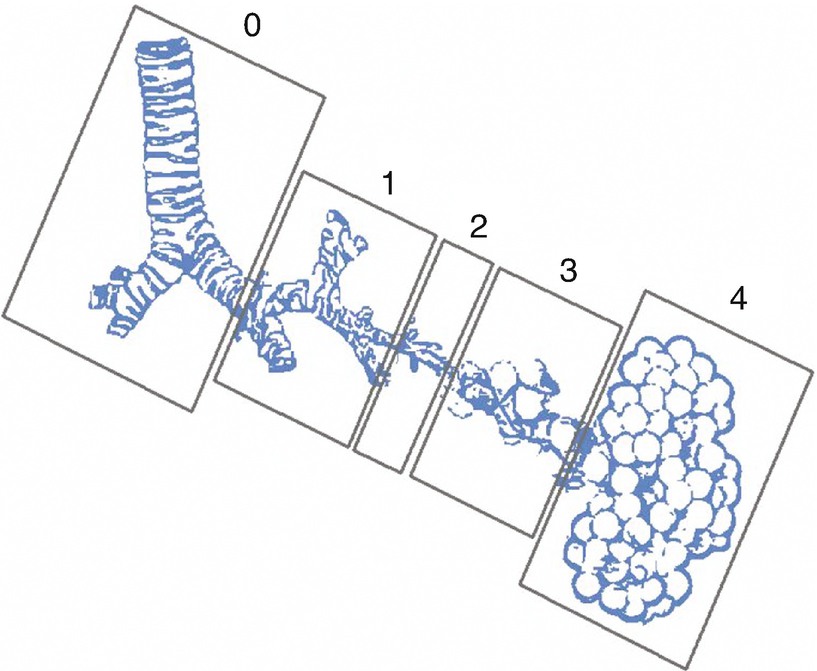
Congenital malformation of the lung airway. Classification of the congenital malformation in the lung airway or cystic adenomatoid malformation, according to the supposed origin during lung development
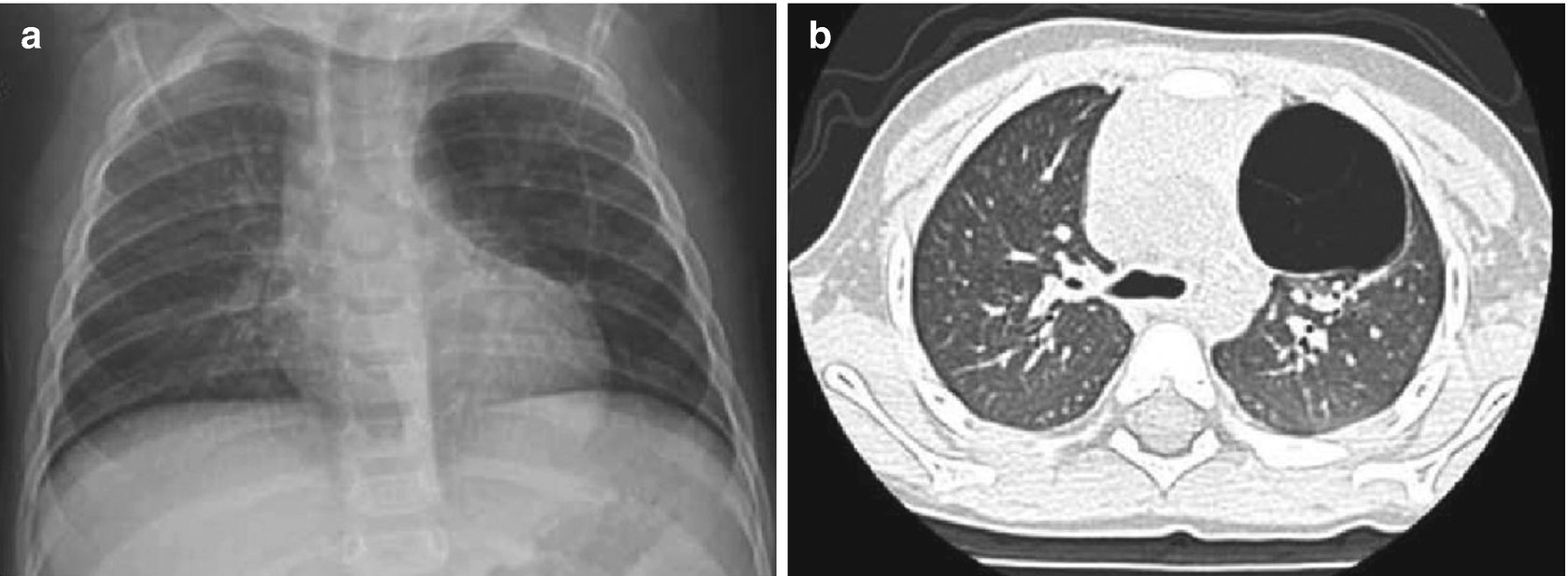
Cystic adenomatoid malformation. (a) Chest X-ray of 1-year-old infant with persistent cough shows a radiolucent region in the superior left lobe. (b) Complementary study of the patient with computerized tomography shows a unique cystic lesion, with fine septations
Lung Sequestration
Lung sequestration is defined by the presence of lung tissue inside or outside the visceral pleural (intra- or extralobar sequestration), with no connection to the normal tracheobronchial path, and characterized by an anomalous blood delivery in the systemic veins. Venous drainage of intralobar sequestration runs toward the pulmonary veins, while the extralobar sequestration runs to the azygous vein. It has been estimated that lung sequestration is a consequence of an anomalous accessory lung bud, which was created in the primitive intestine that descends toward the caudal along with the esophagus. Extralobar sequestration may be related to other esophageal and bronchial malformations, as well as diaphragmatic defects. Most lung sequestration cases do not present symptoms during the neonatal period, and they present as an incidental image in a routine chest X-ray. They are usually located in the inferior lobes: 70% are in the left inferior lobe; 10% are under the diaphragm; and in 20% of the cases arterial irrigation comes from the infradiaphragmatic aorta. In infants, the most frequent presentation form of lung sequestration is the presence of recurrent pneumonia, which may cause localized bronchiectasis, and a particular complication is congestive heart failure, which is not present in cystic adenomatoid malformation, and is caused by the presence of aberrant circulation, and in some cases, by a significant shunt.
Anatomical extralobar sequestration, but with cystic adenomatoid malformation histology
Extralobar sequestration and cystic adenomatoid malformation in the same patient
Cystic adenomatoid malformation in one lobe, but with systemic irrigation
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


