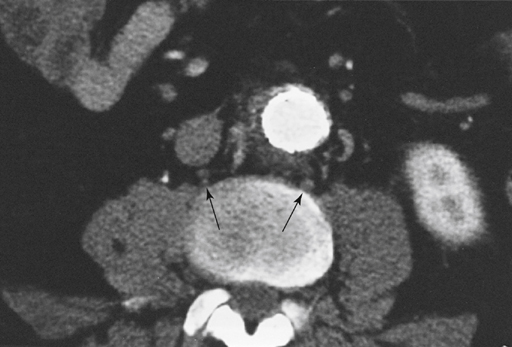
Preganglionic sympathetic fibers that provide outflow to the lower extremities arise from cell bodies in the lateral gray substance of spinal cord segments T10 to L3. These fibers emerge by way of the anterior spinal roots and reach the sympathetic chain through the white rami communicantes. After synapsing with ganglionic cells, the postganglionic fibers pass through the gray rami communicantes to join somatic nerves. These nerves are then distributed to the peripheral blood vessels and sweat glands. Sympathetic innervation of the leg passes through the L1–L4 ganglia. The sympathetic trunks enter the abdomen as paired structures lying on the anterolateral region of the vertebral bodies. This places the left and right trunks behind the aorta and vena cava, respectively (Figure 1).
Lumbar Sympathectomy for Lower Extremity Ischemic Ulcers
Anatomy and Physiology
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


