Severe hypokalemia in the absence of other electrolyte abnormalities, the result of diarrhea, caused striking electrocardiographic changes, generalized weakness, flaccid paralysis of the lower extremities, and biochemical evidence of mild skeletal and cardiac rhabdomyolysis in a 33-year-old man. Repletion of potassium reversed all abnormalities in 24 hours.
A 33-year-old laborer had 6 to 8 beers after work. He awakened at 3 a.m . the next morning to urinate and fell because his legs would not support him. His arms were weak as well. He did not lose consciousness, hit his head, or have any other symptoms. When the paralysis did not improve, some 8 hours later he was brought to the emergency department where an electrocardiogram was recorded ( Figure 1 ).
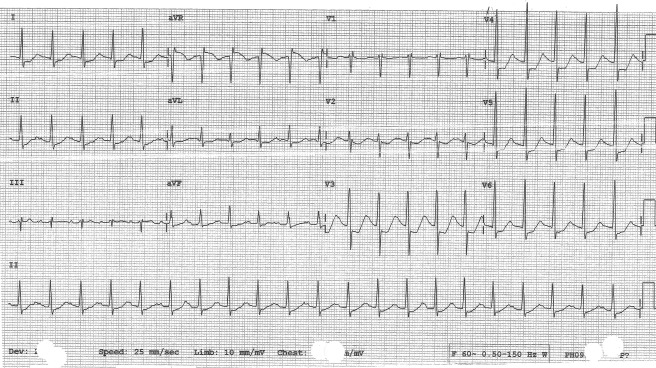
The electrocardiogram showed sinus tachycardia at a rate of 128 beats/min. The most striking features were widespread marked ST-segment depression with broad tall T waves and reciprocal changes in lead aVR. Although the changes could have been interpreted as signs of diffuse subendocardial ischemia/injury, they were actually the result of severe hypokalemia (serum potassium 1.7 mEq/L, reference 3.5 to 5.5). What appeared to be large T waves were instead large U waves superimposed on the T waves.
This patient’s medical history was positive for penicillin allergy and the consumption of 4 to 6 beers on weekends. He used no prescription or over-the-counter medications and no dietary supplements. He had no relevant family history. Of the legion of causes of hypokalemia, this patient’s only recognizable one was diarrhea with 4 to 6 stools per day for the past 3 days with the frequency slowing down the day of admission.
Physical examination revealed only sinus tachycardia and decreased muscle tone and strength bilaterally, especially in the lower extremities. He was unable to walk. A toxicology screen of his urine was negative, and a computed tomographic scan of his head and neck was normal. An echo/Doppler study was normal except for trivial mitral and tricuspid valvular regurgitation and a minimally elevated pulmonary arterial systolic pressure (37 mm Hg).
As serum potassium falls <3.0 mEq/L, muscle weakness and generalized fatigue occur, and at extremely low levels, paralysis and/or rhabdomyolysis may develop. This patient’s serum creatine kinase on admission was 542 U/L (reference 20 to 200). Gastrointestinal smooth muscle and cardiac muscle may also be affected. Fortunately, the patient had no arrhythmias, but his serum troponin I was slightly elevated (0.517 ng/ml, reference <0.034).
Did the large amount of beer contribute to the hypokalemia? Possibly. Many if not most persons drinking large amounts of beer eat a considerable portion of salty food. Acute ingestion of sodium salts may result in kaliuresis and may have added to the effects of the diarrhea in producing hypokalemia in our patient.
The patient’s potassium was repleted, and within 24 hours, his serum potassium was 4.7 mEq/L. Other laboratory studies were normal or nearly so, and his electrocardiogram was normal. He had no symptoms and was discharged home.
Disclosures
The authors have no conflicts of interest to disclose.
Dr. Rodriguez completed his cardiovascular disease fellowship at Louisiana State University Health Sciences Center in New Orleans and currently is finishing a cardiac electrophysiology fellowship at the UCLA/Good Samaritan Program in Los Angeles, California.
See page 1609 for disclosure information.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


