Lower-extremity arterial disease involves a spectrum from intermittent claudication to limb-threatening ischemia. Up to 20% of those over the age of 55 have some degree of peripheral arterial occlusive disease (PAOD). Intermittent claudication, or functional ischemia, of the lower extremities is the most common manifestation of this PAOD. The term claudication comes from the latin claudicatio, “to limp.” Limb-threatening ischemia occurs when there is tissue loss, such as ulceration or gangrene, or ischemic rest pain. Another term used to describe this is critical limb ischemia. Causes may include continual progression of chronic atherosclerosis or acute processes such as plaque rupture with thrombosis, or embolism. As the term limb-threatening ischemia indicates, if treatment is not pursued, there is a high likelihood of amputation.
Patients with claudication may limp or claudicate for several reasons. The patient’s calf muscles may develop cramping pain with walking. The hip and thigh muscles may cramp or tire. Walking also may be limited because of a feeling of diffuse lower-extremity weakness, numbness, and heaviness. Although claudication usually is associated with vascular disease, degenerative hip disease or conditions of the spine such as spinal stenosis, or “pseudoclaudication,” may cause similar symptoms. Therefore, in the evaluation of lower-extremity claudication, the physician must first question the underlying etiology. Is the claudication caused by arterial occlusive disease or some other problem? The history and physical exam often can answer this question (see Chapter 4). Noninvasive testing, including resting segmental pressures (e.g. ankle-brachial indices; ABI), exercise “stress” segmental pressures, accompanying pulse volume recordings (PVR), and duplex ultrasound of the aortoiliac, femoropopliteal, and tibial segments, provide objective data to support or refute the clinical impression (see Chapter 6).
If the initial evaluation suggests arterial occlusive disease as the cause of intermittent claudication, the next question concerns how management proceeds. Which levels of the arterial system are involved? Should therapy be medical, or should a procedure such as percutaneous balloon angioplasty, stenting, or atherectomy be entertained, or should an operation be recommended? And, if surgery is chosen, what operation should be performed? If acute or limb-threatening ischemia is present, what is the likely etiology? How quickly is assessment and treatment needed?
This chapter delineates answers to these issues and gives global evaluation, diagnostic, and therapeutic insight for assessment of those with lower-extremity vascular disease.
I. Patterns of disease.
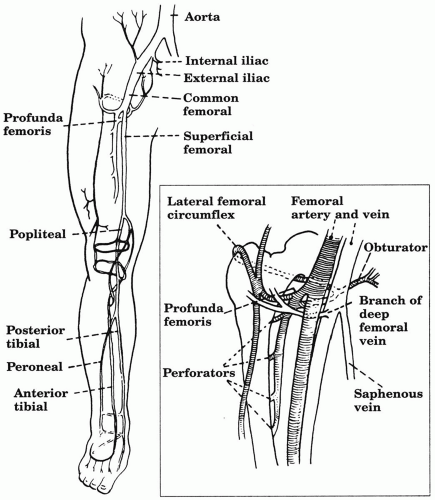
Vascular claudication of the lower limb generally is caused by an arterial stenosis or occlusion in two general regions (Fig. 14.1). A common location of stenosis or occlusion in the superficial femoral artery is at the adductor canal. In diabetics, infrainguinal disease classically involves the tibial arteries. The other large anatomic category of claudicants has occlusive disease localized primarily to the distal abdominal aorta and iliac arteries with open distal arteries, this is termed aortoiliac disease. Over time, collateral branches in the groin and around the knee become well developed when occlusive disease occurs (Fig. 14.1).
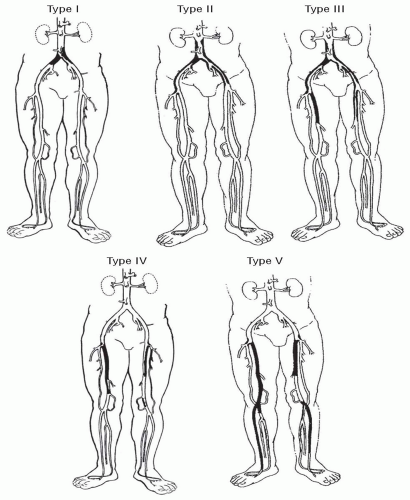
Patient history, physical examination, and noninvasive segmental leg pressures and pulse volume recordings usually can identify the primary location and objectify the severity of disease. Since therapeutic decisions are influenced by the location of occlusive lesions, we categorize patients into five patterns of peripheral arterial disease (Fig. 14.2).
A. Aortoiliac disease (type 1 and type 2).
Type 1, the least common pattern (10% to 15%), is limited to the distal abdominal aorta and common iliac arteries. Patients with focal aortoiliac disease are characteristically between the ages of 35 and 55, with a low incidence of hypertension and diabetes but a high frequency of heavy cigarette smoking and hyperlipidemia. There has been an alarming increase in premature atherosclerotic aortoiliac disease in younger women (age 35 to 50) who have smoked since adolescence. These patients generally complain of proximal lower-extremity claudication involving the hip and thigh muscles with progression to the calf muscles. In about 15% of such patients, however, the claudication affects only the calves. Diminished femoral pulses and femoral bruits are characteristic physical findings. Weak pedal pulses often are palpable, since the femoropopliteal system is open. Some men have the tetrad of bilateral hip and buttock claudication, impotence, leg muscle atrophy and absent femoral pulses, which is called Leriche’s syndrome. Patients with type 2 disease (20%) have aortoiliac atherosclerotic lesions that also involve the external iliac arteries extending to the groin. Final definition of whether the patient has type 1 or 2 aortoiliac disease must be made by imaging. Classic findings of peripheral arterial disease may be present in either of these two categories of proximal aortoiliac occlusive disease as well as any of the remaining three categories to be discussed. Such findings include atrophic skin, dray and flaky skin include atrophic skin, dry and flaky skin (due to poorly functioning skin appendages), and hypertrophic toenails due to an ischemic cuticle. Dependent rubor is a late finding but is classic.
Figure 14.1. Arterial anatomy of the lower extremity. The most common locations of atherosclerotic occlusive disease causing claudication are the aortoiliac region and the superficial femoral artery. Enlarged drawing of the femoral region demonstrates the major collateral channels of the profunda femoris artery. Enlarged drawing of the popliteal region shows the genicular collateral network around the knee connecting the distal SFA to the infragenicular arteries.
B. Combined aortoiliac and femoropopliteal disease (type 3).
The majority of patients with lower-extremity claudication (66%) have combined aortoiliac and femoropopliteal disease (type 2), which usually occurs in patients with multiple cardiovascular risk factors: smoking, hypertension, hyperlipidemia, and sometimes adult-onset diabetes mellitus. These patients usually have more incapacitating, higher grade claudication than is seen in aortoiliac or femoropopliteal disease alone and often progress to more severe ischemia problems, such as rest pain, foot ulcers, or gangrene (i.e., critical ischemia).
C. Isolated femoropopliteal disease (type 4).
Patients with isolated femoropopliteal disease generally present with calf claudication that starts after the patient walks for some time and is relieved by stopping for a few minutes. These patients are older (age 50 to 70) and have a higher prevalence of hypertension, adult-onset diabetes mellitus, and associated vascular disease of the coronary and carotid vessels than those with aortoiliac disease. Like patients with aortoiliac disease, they frequently are cigarette smokers. They generally have good femoral pulses but no palpable popliteal or pedal pulses. Their claudication usually is improved by a supervised walking program and remains stable for long periods of time if significant proximal aortoiliac disease is not present. In fact, the following observations support initial nonoperative management: Patients over 60 years of age with superficial femoral artery occlusive disease (a) have a low likelihood of limb loss (2% to 12% in a 10-year follow-up) if followed closely on conservative treatment, (b) can expect improvement in symptoms (80%) if the initial ABI is greater than 0.6, and (c) should undergo evaluation for percutaneous treatment or reconstructive surgery if the ABI falls below 0.5. Five-year survival is 70% to 80%, and only 10% will require surgical revascularization.
Figure 14.2. Patterns of arterial occlusive disease of the lower extremitites. Type 1 is limited to the distal abdominal aorta and common iliac arteries. Type 2 is aortoiliac, involving the aorta, common iliacs and also the external iliacs. Type 3 involves these areas and the femoropopliteal region. Type 4 is isolated femoropopliteal disease with preserved aortoiliac inflow and poplitealtibial outflow. Type V is combined disease of the femoropopliteal and more distal tibial arteries.
D. Femorpopliteal-tibial disease (type 5).
These patients are at highest risk of limb loss over time. This is due to the poor long-term outcomes with revascularization treatments for disease in the tibial vessels. Furthermore, within this particular pattern of disease patients are usually older (over 65) and have a significant prevalence of diabetes mellitus, smoking, and lipid abnormalities, all of which are significant factors in disease progression. Diabetes in particular has been implicated in disease progression and is causative in infrapopliteal disease. Some within this group have classically spared aortoiliac and femoropopliteal segments with diffuse, significant tibial disease. These are usually poorly controlled diabetics and noted to be of Hispanic and Native American ethnicities.
II. Common clinical scenarios.
Understanding the spectrum of lower-extremity ischemia and how it is classified is vital. This practical classification helps to break down and define how the limb ischemia is approached therapeutically. Chronic limb ischemia (Table 14.1) and acute limb ischemia (Table 14.2) classifications are available and reveal the spectrum of chronic disease and help define the imminent viability of the limb, respectively. Lower limb ischemia in the great majority of cases is due to atherosclerotic disease, but a large spectrum of vascular diseases may cause the symptoms (Table 14.3).
A.
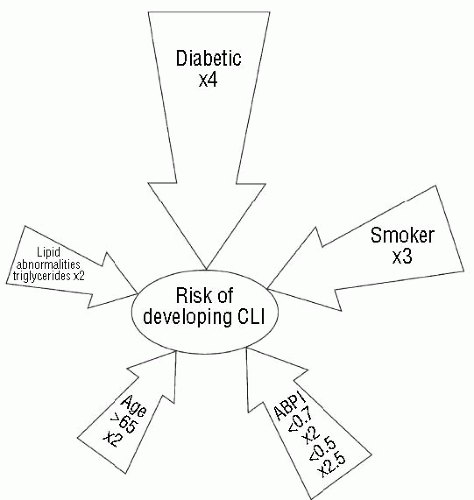
Claudication (grade I; categories 1-3; Table 14.1) is a reproducible, consistent pain, ache, fatigue, heaviness, numbness and/or weakness of muscle groups due to exercise-induced ischemia. Symptoms are absent at rest and abate when exercise is stopped. In general, the symptoms occur in the muscle groups one level beyond the significant disease. Thus, calf claudication alone usually indicates superficial femoral artery disease. The addition of the thigh and buttock muscles points to aortoiliac disease. The disappearance of the symptoms is not positional as opposed to neurogenic claudication. The natural history of intermittent claudication due to arterial insufficiency is a benign one in general. Only 4-5% of those with true vascular claudication progress to a limb-threatening stage. Most actually die of associated cardiovascular morbidity, rather than from factors related to their leg ischemia. Similarly, many patients with asymptomatic but identified atherosclerosis of their lower-extremity arteries do not progress to develop symptoms if their condition is managed carefully. This being said, there are certain factors associated with advancement of PAOD to the critical point (Fig. 14.3).
B. Critical ischemia.
Ischemic rest pain in the lower extremity may be the first symptom of severe ischemia (grade II, category 4; Table 14.1). There are many causes of leg and foot pain in which arterial perfusion to the foot may be normal. These include diabetic neuropathy, arthritis, venous insufficiency, and causalgia-type complex regional pain syndromes. Specific features suggest pain to be of ischemic origin. Ischemic rest pain is sharp and localized primarily to the forefoot below the ankle and the foot usually has dependent rubor and elevation pallor. Not uncommonly, patients are awoken by the pain at night and dangle their foot for relief. Palpable pulses are absent.
(Adapted from: Inter-society Consensus for the Management of Peripheral Arterial Disease (TASC II). J Vasc Surg. 2007;45(suppl S):S29A.)
The reason ischemic rest pain is classified as limb threatening is clear. Once perfusion is so poor that rest pain develops, 95% of people will loose the limb within a year unless revascularization is instituted. An interesting group of patients has recently been identified as having “subcritical” ischemia. These patients have severe disease with no apparent symptoms, usually due to inactivity, and a resting ankle pressure <50 mm Hg with a toe pressure <40 mm Hg. Some have nonspecific symptoms in their leg with exertion, which may be attributed to the degree of their ischemia but this is usually not clear. They are at increased risk for progression to limb loss as well, but almost one-third will still have their limb at one year without revascularization, and with comorbidities medical management may be appropriate.
Table 14.2. Categories of acute limb ischemia
Category
Description
Capillary refill
Muscle weakness
Sensory loss
Arterial Doppler
Venous Doppler
I. Viable
Not immediately threatened
Intact
None
None
Audible
Audible
II. Threatened
a. Marginally
Salvageable if promptly treated
Intact, slow
None
Minimal (toes) or none
Often audible
Audible
b. Immediately
Salvageable with immediate revascularization
Very slow or absent
Mild, moderate
More than toes, associated with rest pain
Usually inaudible
Audible
III. Irreversible
Major tissue loss, amputation regardless of treatment
Absent (marbling)
Profound, paralysis (rigor)
Profound. anesthetic
Inaudible
Inaudible
(Adapted from Inter-society Consensus for the Management of Peripheral Arterial Disease (TASC II). J Vasc Surg. 2007;45(Suppl S):S41A.)
Figure 14.3. Influence of risk factors on the development of critical limb ischemia (CLI) in those with peripheral arterial occlusive disease (PAOD). ABPI, ankle-brachial pressure index. (From Inter-society Consensus for the Management of Peripheral Arterial Disease [TASC II]. J Vasc Surg. 2007;45(suppl S):S10A with permission.)
Ischemic rest pain usually does not occur unless the patient has at least two hemodynamically significant arterial occlusive lesions (e.g., at least two levels of disease). Most individuals with rest pain will have one of two distinct anatomic patterns of occlusive disease that must be defined before an appropriate therapy can be selected:
Nonhealing ulcers of the distal foot may also be the result of arterial ischemia (grade III, categories 5 and 6; Table 14.1). Even with arterial perfusion, healing may be prevented by infection of bone or soft tissue, pressure from improper footwear, foot malformation, or improper medical treatment. In this situation the metabolic demand of the local process outstrips the arterial supply. A good history and physical should provide information for sorting out the reasons for poor healing. The sensory neuropathy associated with long-term diabetes makes diabetic patients susceptible to neuropathic foot ulcers. Such patients may not feel the initial sore and therefore not present until the ulcer is deep and infected.
D. Critical ischemia.
Gangrene is a classic sign of ischemia in the skin and subcutaneous tissue (grade III, categories 5 and 6; Table 14.1). Dry gangrene is characterized by a noninfected black eschar, whereas wet gangrene has tissue maceration and purulence.
E.
Microemboli cause bluish, mottled spots scattered over the toes (blue toe syndrome), which may be painful. They also may be mistaken for local traumatic bruises, and their true significance overlooked. Microemboli may originate from any point in the proximal arterial system, most commonly from the heart, aneurysms, or ulcerated plaques.
F.
Acute arterial ischemia (Table 14.2) is characterized by the sudden onset of extremity pain, pallor, paresthesia, pulselessness, poikilothermia, and sometimes paralysis. If the patient has a history of claudication or previous lower-extremity arterial graft, the symptoms may be caused by thrombosis of a stenotic artery, usually from acute atherosclerotic plaque rupture, or the arterial graft. If the patient previously had no symptoms of peripheral vascular disease, the acute ischemia is more likely embolic. The embolic source is usually the heart, followed distantly by more proximal atherosclerotic disease.
III. Management.
A. Claudication/functional ischemia.
The following principles are crucial in determining the best treatment for a patient with intermittent vascular claudication. For most patients, initial treatment is nonoperative. As mentioned, only 5% to 10% of patients with claudication will require amputation of an extremity due to progression of the disease in 5 years, most of whom continue to smoke or who have diabetes mellitus. Lower-extremity imaging can be accomplished by CTA, MRA, or duplex ultrasound. Arteriography should be viewed as an invasive intent to treat and is not usually necessary in the majority of patients with recent onset vascular claudication.
1. Determination of initial treatment is based on the duration, disability, and progression of the claudication. Initial management also is influenced by the patient’s medical condition.
a. Duration. If the leg claudication is of recent onset and is not incapacitating, a trial period of nonoperative therapy is indicated without the need for an imaging. This approach is recommended particularly for patients who are suspected of having a recent superficial femoral artery occlusion. Although they may experience sudden severe calf claudication when the artery occludes, their claudication usually improves in 6 to 8 weeks if profunda femoris arterial collaterals are well developed. In general, we prefer to follow patients with recent onset of claudication for at least 3 to 6 months to determine whether the claudication will stabilize, improve, or worsen.
b. Disability. We generally ask two important questions of the patient about the disability imposed by the leg claudication: Does the leg claudication prevent normal activity, especially the performance of essential daily activities or a job? Does the claudication limit leisure activities that the patient enjoys? In our experience, the answers to these two questions are more helpful in determining patient management than is the distance the patient can walk before he or she is stopped by claudication, but this test may provide helpful insight to the severity of disease.
c. Progression. It is extremely important to determine whether the claudication is stable or progressing. Patients who have noted rapid progression of claudication over 6 months to 1 year are more likely to need arterial reconstruction than are stable claudicants. Patients with progressive claudication also are more likely to appreciate any relief that revascularization may provide.
d. Assessment of the patient’s general medical condition is essential for determining the proper initial management of claudication. Elective operations for intermittent claudication should be reserved for patients who appear to have a low risk of mortality (2% to 3%) and morbidity. This assessment is discussed in detail in Chapter 8. Patients with multiple medical problems and stable leg claudication should be followed until symptoms become incapacitating or the limb is threatened by progression to rest pain, nonhealing ulcers, or gangrene (i.e., critical limb ischemia).
2. Nonoperative management includes a supervised, structured walking program and control or elimination of cardiovascular risk factors. Nonoperative management includes regularly scheduled follow-up assessments with noninvasive surveillance. This usually includes either ABIs or segmental pressures and PVRs. This also allows for ongoing assessment of the patient’s peripheral vascular system as many people with PAOD have concomitant cerebrovascular, coronary, and aneurysmal disease.
a. Regular lower-extremity exercise increases metabolic adaptation to ischemia due to walking and may enhance collateral blood flow. The result is stabilization or improvement of claudication. A variety of exercise programs can alleviate claudication. A relatively simple program that has helped 80% of our patients emphasizes the following concepts:
(1) Patients are asked to set aside a definite period and frequency for exercise in addition to normal daily activities (e.g., 30 minutes, 3 to 5 days per week). Exercise every day may be too much activity for many older patients; consequently, an everyother-day exercise program is ideal.
(2) Patients are instructed to walk at a comfortable (not too fast) pace and stop for a brief rest whenever claudication becomes severe.
(3) This walk-rest routine should be continued for 30 minutes. As the leg muscles adapt to anaerobic metabolism, the frequency and length of rest stops will decrease. After 6 to 8 weeks, most claudicants can double or triple their comfortable walking distance. In bad weather, the patient may use an indoor treadmill, walk inside a shopping mall, or use a stationary exercise bicycle.
b. Risk factor control.Chapter 7 describes the important and critical cardiovascular risk factors associated with PAOD. Smoking cessation, control of hyperlipidemias, diabetes mellitus, hypertension, and weight reduction are imperative if nonoperative management is to have a maximal effect. Failure of nonoperative management in the claudicant is usually due to the inability to quit smoking and control these other factors.
c. Pentoxifylline (Trental, Hoechst Marion Roussel, Kansas City, MO, U.S.A.) was the first drug approved by the U.S. Food and Drug Administration for the treatment of intermittent claudication. This rheologic agent is a methylxanthine that reduces blood viscosity by improving red blood cell membrane flexibility and inhibits platelet aggregation. Although the benefits of pentoxifylline are still debated, a recent meta-analysis concluded that the drug resulted in an average 29 m increase in initial claudication distance and a 48 m increase in absolute claudication distance compared to placebo.
d. Cilostazol (Pletal, Otsuka Pharmaceuticals, Rockville, MD, U.S.A.) is a more recent medication for intermittent claudication. It is a phosphodiesterase III inhibitor with vasodilator and antiplatelet activity. Three randomized trials have shown improvements in initial claudication distance and absolute claudication distance in the treated groups compared with placebo.
In our practice, pentoxifylline, 400 mg two or three times daily with meals, or cilostazol, 100 mg twice daily, have been combined with a walking program and smoking reduction for selected patients with mild to moderate claudication. If walking is improved after 6 to 8 weeks, the drug is often stopped to ascertain whether exercise and abstinence from tobacco will maintain improvement. If claudication worsens, the drug may be restarted. Common side effects of pentoxifylline are gastrointestinal upset and dizziness. Some patients can tolerate only 400 mg twice daily. For cilostazol, the most common side effects are headache and diarrhea. Cilostazol is contraindicated in patients with class III or IV congestive heart failure and a significant arrhythmia history. If used, the dose should be reduced to 50 mg twice a day for those on calcium channel blockers, ketoconazole, or erythromycin derivatives as these inhibit cilostazol’s hepatic metabolism by the P-450 system. Increased drug concentrations potentiate its risk of atrial arrhythmias.
We emphasize that drug therapy with pentoxifylline or cilostazol cannot prevent the need for revascularization in patients with severe progressive claudication or critical ischemia.
3. Indications for invasive therapy in a claudicant. Patients must be selected carefully for percutaneous therapies or surgery for lower-extremity claudication. Impairment of occupational performance and significant lifestyle limitation on a low-risk patient are reasonable indications. In this situation, it is important that a favorable anatomic situation for percutaneous or surgical reconstruction be present. The best results are obtained when the occlusive disease is localized to the aorta and iliac arteries with open distal vessels. Isolated superficial femoral artery disease with good (two or more tibial vessels continuous to the foot) runoff is also a favorable anatomic lesion for treatment.
We generally discourage elective arterial reconstruction for stable claudication if the primary disease is (a) combined severe, diffuse aortoiliac and severe femoropopliteal arterial disease or (b) severe below-the-knee popliteal and tibial artery disease. Aortoiliac angioplasty/stenting or an aortofemoral bypass in the setting of a patent, large, well-collateralizing profunda femoris artery may significantly improve many patients. However, without this type of runoff the immediate or staged addition of a femoropopli teal bypass may be necessary to significantly relieve claudication when multilevel occlusive disease (type 3) exists. Thus, aortofemoral reconstruction for claudication in patients with combined aortoiliac and femoropopliteal disease should be recommended only when claudication is rapidly progressing and the aortoiliac disease has advanced to critical stenoses or occlusions and it is clear that normalizing inflow with reasonable outflow is likely to provide im provement in activity level. Likewise, due to reduced durability compared to above-knee reconstructions, below-the-knee femoropopliteal or femorotibial bypasses should be limb salvage procedures, and rarely should they be used to treat claudication alone.
Currently, the rapid advancement and use of endovascular therapies has led to readdressing the indications for intervention for claudication. In general, proponents of endovascular therapies for claudication believe that such interventions have lower associated risk to the patient and ultimately improve activity levels. In addition these proponents point out that in the majority of cases endovascular therapies do not “burn bridges” for future endovascular or open surgical reconstruction. At this time, as bodies of evidence are accumulating, we believe there is no definitive evidence that indications for intervention in claudication should be changed based solely on the availability of endovascular therapies (e.g., just because it can be done doesn’t mean it should be done).
4. Preoperative evaluation.
a. The principles of assessing operative risk and stabilizing chronic medical problems are discussed in Chapter 8. Mortality for percutaneous, endovascular therapy should be negligible. Operative mortality for elective aortoiliac reconstruction or femoropopliteal bypass for claudication should not exceed 2-3%. The primary risk to life during vascular reconstructions is coronary artery disease. Significant coronary artery disease exists in at least 40% of patients with peripheral vascular disease. In general, we recommend that the necessary surgical procedures for significant coronary artery disease be performed before elective vascular intervention is attempted.
b. Before elective surgery, patients should be asked to make a commitment to stop smoking and to not resume tobacco use after recovery. They should be informed that the chance of graft failure approaches 30% in patients who continue to smoke regularly. Elective reconstruction for claudication in active smokers should be eschewed, but can be entertained once a significant and progressive reduction in smoking has occurred to the point of just a few cigarettes a day. Most of these individuals will quit completely after hospitalization.
c. Lower-extremity arteriography is performed only after the decision has been made to intervene with arterial reconstruction or percutaneous therapy. In our practice, we liberally use duplex ultrasound to delineate arterial disease prior to arteriogram to aid in determining the possibility of an endovascular revascularization option prior to arteriography. This is purely lab dependent. Intravenous contrast may, therefore, be minimized if inflow and outflow segments do not need dedicated arteriographic interrogation prior to intervention. Others use CTA and MRA in a similar manner, while some proceed directly to arteriography and make an on-table determination of therapeutic options. Ideally, at least a one-day delay should be allowed before open surgical revascularization to ensure that renal function does not deteriorate after the contrast load from the angiogram. Endovascular therapy can be instituted at the same sitting as diagnostic arteriography, or delayed in a staged fashion several days to weeks later.
Table 14.4. Aortofemoral graft for multilevel occlusive disease: Predictors of success and need for distal bypass
Emphasis of Evaluation
Predictors of Good AF-Only Result
Predictors of Need for Distal Bypass
Proximal disease
Absent or severely reduced femoral pulse
“Normal” femoral pulse
Severe stenosis/occlusion (arteriogram) (positive femoral artery pressure study)a
a Femoral artery pressure study. An iliac stenosis is significant when the resting pressure gradient across iliac segment is greater than 5 mm Hg or falls more than 15% after reactive hyperemia or directed injection with papaverine or nitroglycerin.
b Index runoff resistance = thigh-ankle pressure difference/brachial pressure
(Adapted from: Brewster DC, Perler BA, Robinson JG, Darling RO. Aortofemoral graft for multilevel occlusive disease: predictors of success and need for distal bypass. Arch Surg 1982;117:1593-1600.)
5. Selection of proper procedure in aortoiliac disease. The choice of operation or endovascular intervention for claudication depends on the general condition of the patient, the extent of the atherosclerotic process, and the experience of the surgeon/interventionalist. The preoperative arteriogram in conjunction with both resting and “stress” femoral artery pressure measurements, using techniques for distal vasodilation to unmask a stenosis, are the best determinants of which procedure to undertake in a given patient (Table 14.4). A well-trained vascular surgeon should understand the indications and limitations for the following procedures: aortoiliac endarterectomy, aortoiliac or aortofemoral bypass graft, femoropopliteal bypass, lumbar sympathectomy, transluminal angioplasty, angioplasty and stenting, and extraanatomic reconstruction such as axillofemoral and femorofemoral bypasses.
a. Aortoiliac endarterectomy. In patients with occlusive disease limited to the distal aorta and common iliac arteries, aortoiliac endarterectomy gives excellent long-term results, provided the patient eliminates or controls his or her vascular risk factors. Endarterectomy is contraindicated in the presence of (a) aortic or iliac aneurysmal disease, (b) aortic occlusion to the level of the renal vessels, or (c) any occlusive disease in the external iliac or femoral arteries. The 5- and 10-year patency rates are 95% and 85%, respectively. However, such focal aortoiliac disease is currently treated in most patients by percutaneous balloon angioplasty and stenting with excellent results at decreased procedural risk. This has relegated endarterectomy to almost a historical setting.
b. Percutaneous transluminal angioplasty/stenting is currently the initial treatment of choice for focal arterial lesions that cause claudication (see Chapter 11). While beyond the full scope of this discussion, the TransAtlantic Inter-Society Consensus documents on the management of PAOD (TASC I [2000] and TASC II [2007]) have provided anatomic recommendations on the use of endovascular revascularization (Fig. 14.4). These communications place the growing literature and changing technology into perspective. Suffice it to say that as atherosclerotic lesions become longer, more tortuous, and completely occluded, the more difficult are the endovascular solutions. Thus, a focal common iliac stenosis of less than 3 cm in length has been a lesion well suited to endovascular treatment (TASC A). Endovascular recanalization of long iliac occlusions and infrarenal aortic disease, and longer severely diseased iliac lengths (TASC C and D) are also commonplace as first-line therapy, yet surgery remains superior. Endovascular therapies, however, will only become more widespread as re-entry technology and stent engineering improves. Owing to their inferior durability, these reconstructions require close serial duplex surveillance and repeat intervention as necessary.
Angioplasty results in the iliac system are enhanced by the addition of stents. Balloon expandable stents are generally used in the common iliac where the plaque burden is usually bulky and significantly involved with calcification. The radial force of these stents is helpful in this case (Chapter 11). In the external iliac artery, self-expanding stents are generally used as they are more flexible in this variably tortuous area. This therapy has provided a primary patency rate of 70-80% at 4 years. Consequently, the primary limitation of aortoiliac endovascular therapy is restenosis, which affects 20% to 30% of patients within 3 to 5 years. These current results indicate that repeated endovascular intervention may be required to achieve satisfactory, long-term relief of symptoms. The impact that newer technologies, such as cutting balloons, cryoplasty, re-entry devices, and both directional and laser-based atherectomy devices, may have on these results remains to be clarified.
Only gold members can continue reading. Log In or Register to continue