Level 2
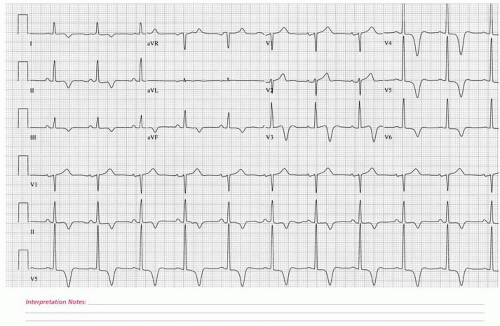
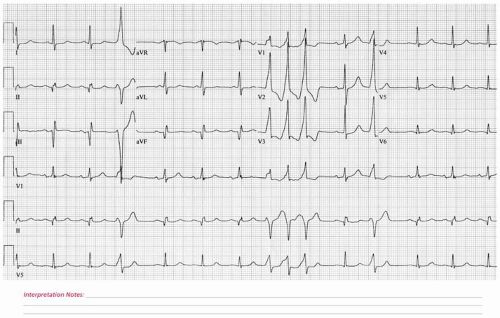
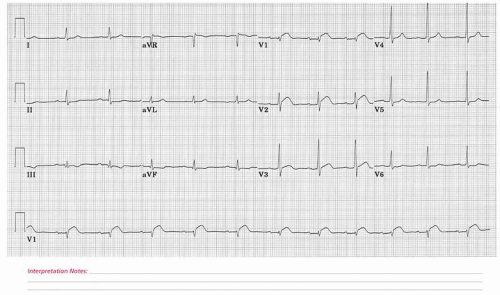
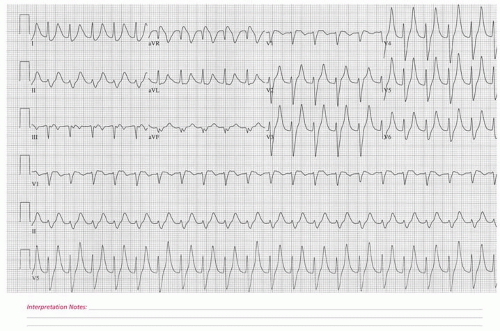
 ECG 169 A 46-year-old female who presents for an initial cardiac electrophysiology evaluation in the setting of paroxysmal tachycardia and presyncope. She had been previously evaluated by her primary care physician at which time an electrocardiogram was obtained and judged to be abnormal. |
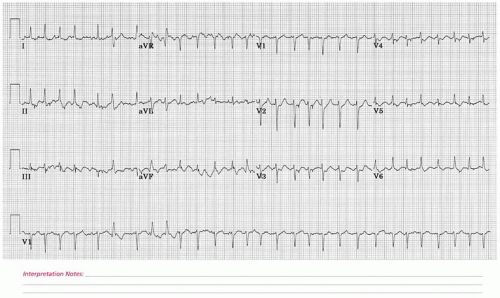
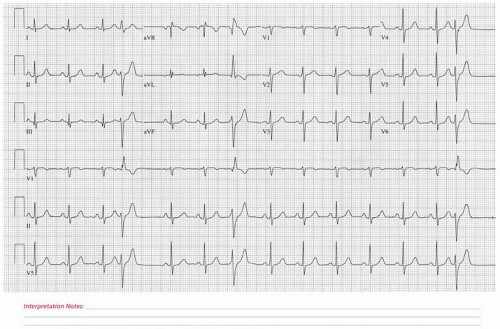
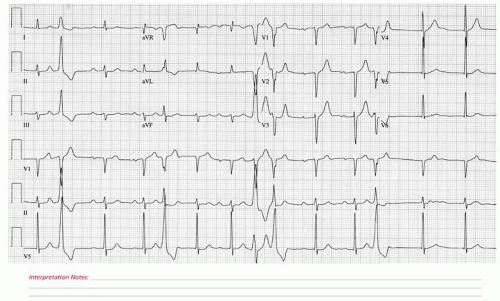
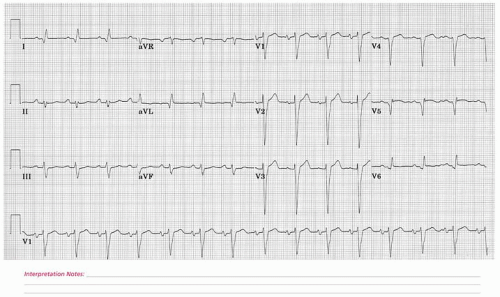
 ECG 170 A 54-year-old female who presents for a routine physical examination. |
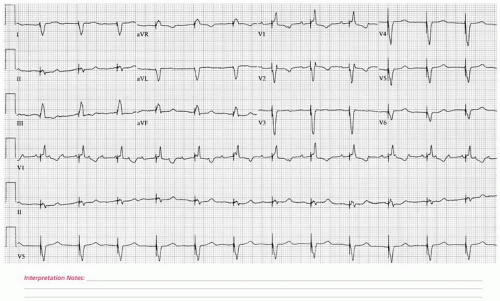
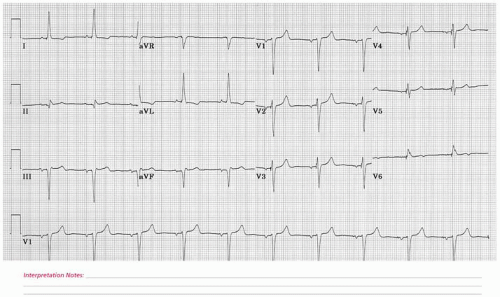
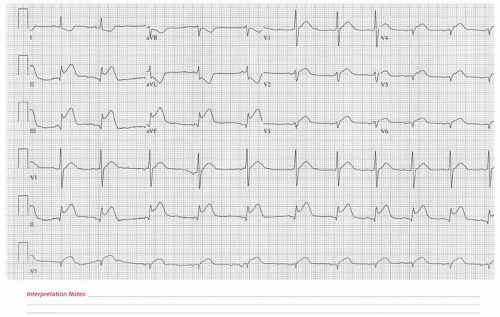
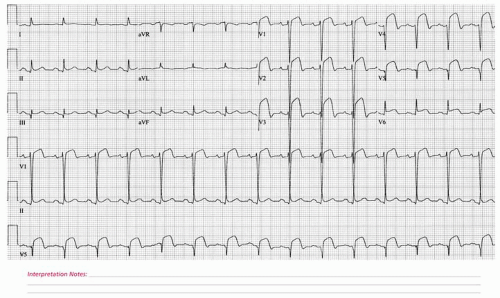
 ECG 171 An 84-year-old woman with a history of hypertension and spinal stenosis who was noted to have a sudden-onset tachycardia during preoperative evaluation. The patient received intravenous verapamil at which time she converted to normal sinus rhythm. Extended-release verapamil was continued without further dysrhythmia recurrence. |
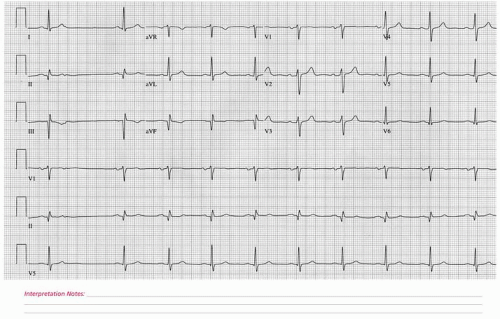
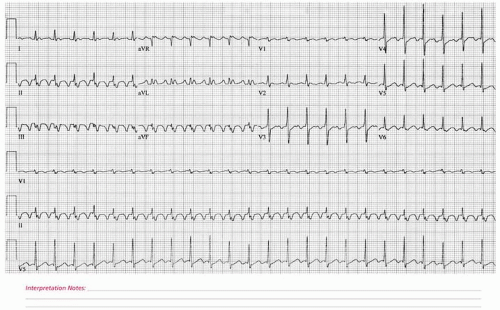
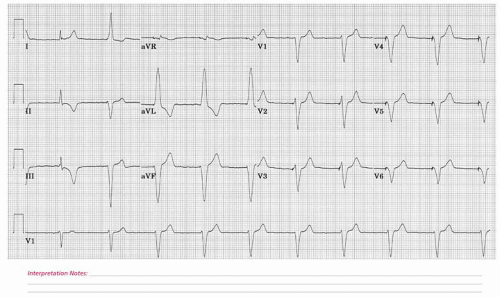
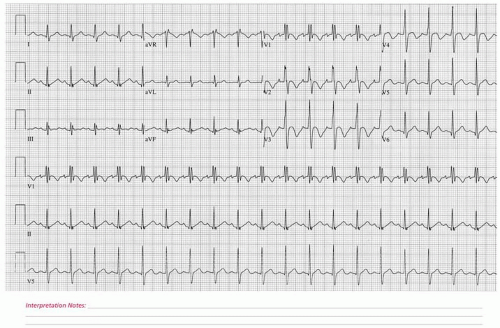
 ECG 172 A 92-year-old female who presented acutely to the emergency room after calling EMS with acute-onset severe anterior chest discomfort and shortness of breath beginning 30 minutes prior to hospital arrival. She was immediately taken to the cardiac catheterization laboratory at which time an acute proximal left circumflex coronary artery occlusion with superimposed thrombus was identified and successfully stented. She was discharged to a long-term care facility 7 days after her initial presentation. |
 ECG 173 A 46-year-old male with a severe episode of anterior chest pain 2 weeks previously who presents to his physician with persistent shortness of breath. |
 ECG 174 A 46-year-old male accepted in-hospital transfer 2 days after the sudden onset of severe anterior chest discomfort with radiation to both arms. Medications at the time of this tracing included metoprolol, intravenous heparin, and aspirin. The patient underwent a cardiac catheterization demonstrating a severe proximal right coronary artery stenosis and subsequent successful percutaneous transluminal coronary angioplasty. |
 ECG 175 A 69-year-old male who is seen in preoperative cardiovascular medicine consultation prior to a planned near-future cystectomy and ileal loop conduit for recently diagnosed bladder carcinoma. Upon questioning, he had been experiencing what he described as a 3-week history of exertional chest heaviness with walking such as one flight of stairs or a slight incline. Given the high suspicion of new-onset angina pectoris in the context of near-future moderate-risk noncardiac surgery, it was decided to proceed directly with a diagnostic left heart catheterization. This demonstrated coronary artery disease including a subtotal obstruction of the proximal left anterior descending involving a moderate-sized branching first diagonal. The patient underwent successful angioplasty to his first diagonal lesion and bare metal stent placement to his proximal left anterior descending coronary artery. Approximately 5 weeks after his coronary artery intervention, he underwent successful and uncomplicated urologic surgery. |
 ECG 176 A 54-year-old female with intermittent palpitations and light-headedness for the past 6 months. |
 ECG 177 A 46-year-old male accepted in-hospital transfer 2 days after the sudden onset of severe anterior chest discomfort with radiation to both arms. The patient received urgent intravenous thrombolytic therapy. Serial cardiac enzyme serum analysis confirmed a large myocardial infarction. Medications at the time of this electrocardiogram included metoprolol, intravenous heparin, and aspirin. The patient underwent a cardiac catheterization demonstrating a severe proximal right coronary artery stenosis and subsequent successful percutaneous transluminal coronary angioplasty. |
 ECG 178 A 60-year-old male with long-standing hypertension and paroxysmal atrial fibrillation admitted to the hospital for sotalol initiation and continuous telemetry monitoring. This electrocardiogram was obtained after his fifth dose of sotalol. The patient did not demonstrate proarrhythmias. The sotalol was discontinued, and his electrocardiogram returned to its normal baseline within 24 hours. |
 ECG 179 A 61-year-old male seen preoperatively prior to a planned lung mass resection. |
 ECG 180 A 76-year-old woman with coronary artery disease who underwent multi-vessel coronary artery bypass graft surgery 1 year prior to this electrocardiogram. She now presents for evaluation of a recent syncopal episode. |
 ECG 181 A 75-year-old male with severe aortic stenosis and severe mitral valve regurgitation, status post bioprosthetic aortic valve replacement and mitral valve repair performed 1 year prior to this 12-lead electrocardiogram. The patient developed recurrent shortness of breath and anemia with a transthoracic echocardiogram and laboratory studies consistent with recurrent perivalvular mitral valve regurgitation and hemolytic anemia. The patient underwent repeat open-heart surgery in the form of mitral valve replacement. This electrocardiogram was obtained on the 4th postoperative day. |
 ECG 182 A 57-year-old male with the acute onset of severe anterior chest discomfort of 45 minutes duration. |
 ECG 183 A 78-year-old male status post remote aortic valve replacement, coronary artery bypass graft surgery, and recurrent transitional cell carcinoma of the bladder who developed this cardiac dysrhythmia during the intravenous administration of a chemotherapeutic medication. |
 ECG 184 A 67-year-old male with severe pulmonary arterial hypertension, long-standing permanent atrial arrhythmias, and decompensated right-sided systolic congestive heart failure admitted to the hospital in the setting of a severely decreased performance status, ascites, and severe bilateral lower extremity edema extending to his thighs. |
 ECG 185 A 63-year-old male with intermittent exertional light-headedness and chest pressure. |
 ECG 186 A 46-year-old woman admitted to the hospital with acute pneumonia and recent-onset perceived rapid heart beating. Her pertinent past medical history includes steroid-dependent polymyositis. A cardiac catheterization performed 1 year before this electrocardiogram demonstrated normal coronary arteries. |
 ECG 187 A 64-year-old female with known severe mitral valve regurgitation secondary to mitral valve posterior leaflet prolapse and flail complicated by complete heart block and permanent pacemaker placement seen in outpatient cardiovascular medicine follow-up. She had been noticing approximately 2 weeks of persistent fatigue and dyspnea upon exertion with a generalized reduction of her functional capacity. |
 ECG 188 A 54-year-old male who presents for a follow-up cardiovascular medicine evaluation in the context of known coronary artery disease. He is feeling well at the present time. |
 ECG 189 A 74-year-old male admitted for evaluation of recurrent syncope. His past medical history is notable for hypertrophic obstructive cardiomyopathy and coronary artery disease. He is status post angioplasty to his left anterior descending coronary artery 1 year prior to this tracing. He also experienced a prior myocardial infarction in the left circumflex coronary artery distribution. |
 ECG 190 A 76-year-old male with recent-onset shortness of breath and exertional intolerance who has been experiencing an overall subjective decline of his daily functional capabilities. This is in the setting of long-standing hypertension, untreated obstructive sleep apnea, diabetes mellitus, and morbid obesity. |
 ECG 191 A 74-year-old male having undergone coronary artery bypass grafting surgery earlier the same day. |
 ECG 192 A 76-year-old male with laryngeal carcinoma admitted urgently to the hospital with upper airway bleeding and new-onset atrial fibrillation with a rapid ventricular response. |
 ECG 193 A 59-year-old male with known ischemic heart disease and a past myocardial infarction who underwent subsequent coronary artery bypass grafting surgery who is seen for outpatient cardiovascular medicine follow-up. He continues to feel well, is not experiencing adverse cardiac symptomatology, and remains active with his full-time work schedule. |
 ECG 194 A 46-year-old male with hypertension who presents for blood pressure follow-up. |
 ECG 195 A 70-year-old male with coronary artery disease and moderately severe left ventricular systolic dysfunction who is status post coronary artery bypass graft surgery in the remote past. He returns for cardiology and pacemaker follow-up. He also has a history of ventricular tachycardia and is status post implantable cardiac defibrillator placement. His medications at the time of this electrocardiogram included captopril, aspirin, metoprolol, furosemide, warfarin, and topical nitroglycerin. |
 ECG 196 A 52-year-old male with recently diagnosed diverticulitis, status post acute operative intervention in the form of a partial colectomy, who is presently recovering in the hospital. The patient has had an uncomplicated hospital course thus far with the exception of experiencing sudden-onset heart palpitations and diaphoresis at which time this electrocardiogram was obtained. |
 ECG 197 A 50-year-old male with metastatic melanoma hospitalized with shortness of breath. |
 ECG 198 A 77-year-old woman status post an acute left middle cerebral artery occlusion and intravenous thrombolytic administration who is now experiencing recurrent atrial arrhythmias. Medications at the time of this electrocardiogram included diltiazem, topical nitroglycerin, and isosorbide mononitrate. An echocardiogram performed during this hospitalization demonstrated moderate left atrial enlargement and normal left ventricular systolic function without evidence of a prior myocardial infarction. |
 ECG 199 A 67-year-old male with long-standing hypertension, left ventricular hypertrophy, and moderate aortic stenosis seen in outpatient nephrology follow-up. The patient has noted increased lethargy recently, unexplained per his account coupled with intermittent shortness of breath and light-headedness. He has not noted syncope. On physical exam, his radial pulse was suspected to be bradycardic, prompting this 12-lead electrocardiogram. |
 ECG 200 A 77-year-old male immediately postoperative mitral valve repair and coronary artery bypass grafting. The patient remains intubated in the surgical intensive care unit. |
 ECG 201 A 50-year-old male who presents to the hospital with a clinical syndrome consistent with crescendo angina. A cardiac catheterization demonstrated a subtotal proximal occlusion of the left anterior descending coronary artery. This stenosis was successfully stented. The patient subsequently presented to the hospital with recurrent chest pain and this electrocardiogram. A repeat cardiac catheterization demonstrated a patent PTCA site; however, a new 90% stenosis of the right coronary artery was found and successfully stented. The patient suffered a small inferior myocardial infarction as serial serum cardiac enzymes were elevated. |
 ECG 202 A 56-year-old female with degenerative osteoarthritis of both knees who is postoperative day 2 bilateral knee replacements. This electrocardiogram was obtained as the patient suspected an irregular heartbeat. She has no known cardiac history. Comorbid conditions included morbid obesity, hypertension, and obstructive sleep apnea. |
 ECG 203 A 56-year-old male who presented to the hospital emergency room with severe anterior chest pressure of 1-hour duration. This electrocardiogram was obtained in the emergency room. |
 ECG 204 A 75-year-old male with a recent history of syncope and permanent pacemaker implantation. Comorbidities include chronic atrial fibrillation and past coronary artery bypass graft surgery. |
 ECG 205 An 84-year-old male with recent-onset chest discomfort and shortness of breath who presented to his primary care physician. An evaluation including both a 12-lead electrocardiogram and transthoracic echocardiogram confirmed normal heart function and severe aortic valve stenosis. A subsequent left heart catheterization demonstrated advanced multi-vessel coronary artery disease. This 12-lead electrocardiogram was obtained on the 2nd open-heart surgery postoperative day. |
 ECG 206 A 67-year-old male admitted via the emergency room with acute chest pain. The patient was taken immediately to the cardiac catheterization laboratory where an acute proximal left anterior descending coronary artery obstruction was identified. Balloon angioplasty and coronary artery stent placement were successfully undertaken. |
 ECG 207 A 30-year-old male with dialysis-requiring renal failure of unknown etiology who presents with leg pain and tingling, a serum calcium of 4.9 mg/dL, and a serum potassium of 6.2 meq/L. Comorbidities include hypertension and a seizure disorder. |
 ECG 208 An 81-year-old male with severe ischemic left ventricular systolic dysfunction, congestive heart failure, and atrial dysrhythmias who returns for a follow-up cardiac assessment. With the exception of generalized fatigue, he feels reasonably well and is able to complete his activities of daily living unassisted. |
 ECG 209 A 66-year-old female with lung cancer undergoing chemotherapy who is acutely hospitalized with nausea, vomiting, and severe dehydration. |
 ECG 210 A 40-year-old male with a history of “an enlarged heart” since a young age who seeks a cardiac evaluation. A prior echocardiogram demonstrated evidence of Ebstein’s anomaly. |
 ECG 211 An 82-year-old male with known coronary artery disease and moderate mitral regurgitation who returns for outpatient cardiovascular medicine follow-up feeling well. He continues on his daily beta-blocker and ACE inhibitor. |
 ECG 212 A 51-year-old female with mitral valve prolapse and severe mitral regurgitation. The patient presents with exertional intolerance, new-onset palpitations, and signs and symptoms consistent with decompensated congestive heart failure. |
 ECG 213 A 68-year-old male with coronary artery disease status post coronary artery bypass graft surgery 2 years prior to this electrocardiogram who re-presents for evaluation of aortic insufficiency. Medications at the time of this electrocardiogram included captopril, furosemide, potassium, and aspirin. |
 ECG 214 A 70-year-old male who returns for cardiovascular medicine follow-up after presenting 2 weeks previously with syncope, complete heart block, and permanent pacemaker implantation. At the present time, he feels well except for some residual pain at the pacemaker site. He has a history of ischemic heart disease and a remote myocardial infarction. |
 ECG 215 A 54-year-old male with dialysis-requiring end-stage renal disease admitted to the medical intensive care unit after presenting to the hospital with acute delirium. |
 ECG 216 A 48-year-old male with multiple prior myocardial infarctions who was admitted recently to the hospital with severe congestive heart failure. The patient subsequently expired. |
 ECG 217 An 83-year-old male who presented to the emergency room with acute-onset severe chest pain of 40 minutes duration. This 12-lead electrocardiogram was obtained upon arrival in the coronary intensive care unit just prior to being transferred to the heart catheterization laboratory. |
 ECG 218 A 16-year-old male admitted to the hospital with a cerebral hemorrhage due to an arteriovenous malformation. He subsequently expired. |
 ECG 219 A 75-year-old male status post a remote anterolateral myocardial infarction and percutaneous transluminal coronary angioplasty of the left anterior descending coronary artery who re-presents with recurrent angina pectoris. Medications at the time of this electrocardiogram included intravenous nitroglycerin, intravenous heparin, metoprolol, and aspirin. |
 ECG 220 A 66-year-old male with a long-standing history of a perceived irregular heartbeat who seeks a cardiac electrophysiology opinion. He has otherwise remained healthy with the exception of hypertension, well controlled on oral medication. He is asymptomatic from a cardiovascular medicine perspective and maintains an active lifestyle. |
 ECG 221 An 85-year-old male with intermittent chest pain and shortness of breath. He underwent permanent pacemaker placement 5 years prior to this electrocardiogram. |
 ECG 222 A 66-year-old male with a long-standing history of atrial dysrhythmias who is status post aortic valve replacement for endocarditis. He returns for an outpatient cardiology follow-up evaluation. Complete heart block ensued necessitating permanent pacemaker placement. |
 ECG 223 A 62-year-old male with severe coronary artery disease including a critical left main stenosis who underwent coronary artery bypass grafting surgery earlier the same day. The patient suffered an acute myocardial infarction approximately 10 days prior to his open-heart surgery. |
 ECG 224 A 62-year-old female with sudden-onset severe chest discomfort and diaphoresis of 90 minutes duration. She was directly admitted from the emergency room to the coronary intensive care unit. |
 ECG 225 A 63-year-old male with an approximate 25-year history of hypertension who presents to the hypertension clinic for further evaluation. He has noticed recent dyspnea upon exertion. Medications at the time of this tracing included lisinopril. |
 ECG 226 A 76-year-old female with a history of hyperlipidemia, hypertension, and osteoarthritis who returns for a primary care follow-up evaluation. At the present time, with the exception of her osteoarthritic symptoms, she continues to feel well including a well-controlled blood pressure. She is devoid of symptoms referable to her heart. |
 ECG 227 A 79-year-old female with intermittent palpitations who is seen preoperatively prior to near-future foot surgery. |
 ECG 228 A 34-year-old woman who is status post ventricular septal defect repair who returns for a right shoulder injury evaluation. Her medications included thyroxine. A cardiac catheterization performed prior to her heart surgery was without obstructive coronary disease. |
 ECG 229 A 74-year-old female with advanced coronary artery disease, severe ischemic left ventricular systolic dysfunction, and complete heart block, status post permanent pacemaker implantation, who is admitted to the hospital in acute decompensated systolic congestive heart failure. At the present time, the patient is resting comfortably after receiving several doses of intravenous diuretics, demonstrating significant clinical improvement since her hospital admission.
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|