Anthracycline therapy is well known for its adverse cardiac effects. However, few studies have been performed of the long-term follow-up of myocardial function in adult survivors of Hodgkin’s lymphoma receiving anthracycline. Two-dimensional speckle tracking echocardiography is an accurate angle-independent modality for the quantification of left ventricular (LV) function. The aim of the present study was to investigate the long-term effect of anthracycline on LV systolic function. Echocardiography was performed in 47 survivors of Hodgkin’s lymphoma 22 ± 2 years after successful mediastinal radiotherapy with (n = 27) or without (n = 20) anthracycline (doxorubicin) treatment and in 20 healthy controls. LV function was assessed by the LV ejection fraction and global longitudinal and circumferential strain. Both patient groups had received a similar dosage of radiation, and doxorubicin was given at a total dose of 309 ± 92 mg. The global longitudinal strain was reduced in patients receiving anthracycline with mediastinal radiotherapy compared to the other group receiving mediastinal radiotherapy alone or combined radiotherapy and regimens without anthracyclines (−16.1 ± 1.9% vs −17.5 ± 1.7%, respectively, p <0.05). Both patient groups had reduced strain compared to the healthy controls (−20.4 ± 1.7%, both p <0.001). The circumferential strain was also reduced in the treatment groups (−18.3 ± 3.2% and −17.8 ± 3.6% vs −22.5 ± 2.1%, both p <0.001). The LV ejection fraction did not differ between the patient groups (55 ± 8% vs 56 ± 6%, p = 1.0) but was reduced compared to that of the controls (62 ± 5%, both p <0.05). In conclusion, myocardial function was reduced in the survivors of Hodgkin’s lymphoma 2 decades after successful treatment consisting of mediastinal radiotherapy with or without chemotherapy. Patients receiving anthracycline therapy had additional negative long-tem effects on LV systolic function.
Left ventricular (LV) function assessed by the LV ejection fraction (LVEF) is well-established as a strong predictor of cardiac morbidity and mortality. Despite its feasibility, the LVEF is not sensitive enough to reveal subclinical or regional myocardial dysfunction. The detection of myocardial dysfunction can be assessed by myocardial strain from 2-dimensional speckle tracking echocardiography (2D-STE) in patients before an evident reduction in the LVEF. Patients with subclinical LV dysfunction have an elevated risk of developing symptomatic congestive heart failure and increased mortality, emphasizing the importance of detecting subtle changes in cardiac function. Using an M-mode technique, our group recently demonstrated LV remodeling in survivors of Hodgkin’s lymphoma 2 decades after treatment with anthracycline and mediastinal radiotherapy. The aim of the present study was to investigate the long-term effect of anthracycline on LV function assessed by 2D-STE.
Methods
A total of 47 long-term survivors of Hodgkin’s lymphoma (51 ± 9 years old) were divided into 2 groups according to previous lymphoma treatment either with or without anthracyclines at the Oslo University Hospital (The Norwegian Radium Hospital, Oslo, Norway) between 1980 and 1988. All patients had also undergone mediastinal radiotherapy. Additional details regarding patient selection and treatment have been published in our previous study of valvular dysfunction in survivors of Hodgkin’s lymphoma. Of the previously reported 51 patients, 3 who had undergone valvular replacement were excluded and 1 who was unavailable during the study period, were excluded. The patient characteristics were similar between the 2 groups ( Table 1 ). The radiotherapy and anthracyclines group included 27 patients who had undergone mediastinal radiotherapy and anthracycline-containing chemotherapy at 28 ± 10 years of age. The other group, radiotherapy and no anthracyclines, included 7 patients who had undergone mediastinal radiotherapy combined with chemotherapy without anthracyclines and 13 patients who had undergone radiotherapy. The mean dosage of anthracycline and radiation are listed in Table 1 . No patient had had known cardiovascular disease or had been taking any cardiac medications before lymphoma treatment. The patients who had undergone a revascularization procedure were regarded as having confirmed coronary artery disease (CAD).
| Variable | Radiotherapy Plus Anthracycline (n = 27) | Radiotherapy and No Anthracycline (n = 20) | p Value |
|---|---|---|---|
| Age (years) | 50 ± 10 | 52 ± 7 | 0.46 |
| Women | 16 (59%) | 15 (75%) | 0.26 |
| Observation after treatment (years) | 22 ± 2 | 23 ± 3 | 0.18 |
| Radiation dosage (Gy) | 41 ± 3 | 41 ± 1 | 0.95 |
| Doxorubicin dose ⁎ (mg) | 309 ± 92 | — | — |
| Systolic blood pressure (mm Hg) | 122 ± 18 | 125 ± 15 | 0.53 |
| Diastolic blood pressure (mm Hg) | 70 ± 10 | 73 ± 10 | 0.35 |
| Heart rate (beats/min) | 83 ± 15 | 87 ± 10 | 0.38 |
| Hypertension † | 8 (30%) | 5 (25%) | 0.73 |
| Diabetes | 1 (4%) | 0 | 0.57 |
| Revascularization for coronary artery disease | 4 (15%) | 2 (10%) | 0.49 |
| Old myocardial infarction | 3 (11%) | 1 (5%) | 0.43 |
| Coronary artery calcium score | 78 (0 ∼ 1971) | 63 (0 ∼ 767) | 0.73 |
| New York Heart Association | |||
| Functional class I | 25 (93%) | 18 (90%) | 0.57 |
| Functional class II | 1 (4%) | 2 (10%) | 0.39 |
| Functional class III | 1 (4%) | 0 | 0.57 |
| Body mass index (kg/m 2 ) | 23.7 ± 3.5 | 24.2 ± 4.1 | 0.66 |
| Cardiac index (L/min/m 2 ) | 3.0 ± 0.6 | 2.9 ± 0.8 | 0.67 |
| Aortic regurgitation ‡ | 16 (59%) | 9 (45%) | 0.33 |
| Mitral regurgitation ‡ | 9 (33%) | 6 (30%) | 0.81 |
| Aortic stenosis ‡ | 2 (7%) | 3 (15%) | 0.36 |
| Laboratory tests | |||
| Total cholesterol | |||
| mg/dl | 200 ± 36 | 213 ± 25 | 0.18 |
| mmol/L | 5 ± 1 | 5 ± 1 | 0.18 |
| High-density lipoprotein | |||
| mg/dl | 39 ± 0 | 39 ± 0 | 0.60 |
| mmol/L | 1 ± 0 | 1 ± 0 | 0.60 |
| Low-density lipoprotein | |||
| mg/dl | 116 ± 39 | 155 ± 39 | 0.10 |
| mmol/L | 3 ± 1 | 4 ± 1 | 0.10 |
| Triglycerides | |||
| mg/dl | 89 ± 89 | 89 ± 0 | 0.70 |
| mmol/L | 1 ± 1 | 1 ± 0 | 0.70 |
| Pro-brain natriuretic peptide (pmol/L) | 37 ± 48 | 29 ± 43 | 0.58 |
| Current medical treatment (n) | |||
| Platelet inhibitor | 5 (19%) | 2 (10%) | 0.35 |
| β Blocker | 7 (26%) | 3 (15%) | 0.30 |
| Calcium channel blocker | 1 (4%) | 2 (10%) | 0.39 |
| Statin | 4 (15%) | 3 (15%) | 0.65 |
| Angiotensin-converting enzyme inhibitor/angiotensin II receptor blocker | 6 (22%) | 1 (5%) | 0.11 |
⁎ Doxorubicin was main anthracycline, including treatment at relapse.
† Blood pressure ≥140/90 mm Hg or use of any antihypertensive medication.
As a reference group for normal values, 20 age-matched (49 ± 13 years), healthy subjects were recruited from the hospital staff. Their heart rate was 68 ± 9 beats/min at the echocardiographic evaluation. No subject had significant valvular dysfunction as determined using echocardiography. All participants provided written informed consent. The study was approved by the Regional Committee for Medical Research Ethics (REK Sør, Oslo, Norway).
The study examinations were performed using a Vivid 7 scanner (GE Vingmed Ultrasound, Horten, Norway), using a phased-array transducer. All images were obtained in the left lateral decubitus position. The cardiac cycles from 3 standard apical views (4-chamber, 2-chamber, and long-axis views) and parasternal short-axis views were obtained using conventional 2-dimensional gray-scale echocardiography. The frame rate was similar among the patients and healthy controls (68 ± 24 vs 74 ± 24 frames/s, respectively, p = 0.39). The digital loops were stored and analyzed using Echopac software (GE Vingmed Ultrasound).
The LVEF was assessed using the biplane Simpson rule. Longitudinal and circumferential strain values were assessed using 2D-STE and grayscale B-mode images. The principles of myocardial strain analysis have been previously described. End-systole was defined as aortic valve closure in the apical long-axis view. The regions of interest were manually outlined at end-systole by marking the endocardial borders in the apical and parasternal projections. A manual adjustment was performed if the automated tracking was suboptimal. Segmental strain was automatically calculated as the average strain values among all local acoustic markers in each segment. Each projection provided 6 segmental values. The global longitudinal strain was determined by averaging all peak negative systolic segmental strain values from 3 standard apical projections. The circumferential strain was averaged from 6 segments. The diastolic function was assessed by e′ (early diastolic velocity at septal mitral annulus) from Doppler tissue imaging and the left atrial volume index and E (transmitral early diastolic filling) deceleration time by Doppler.
Coronary artery calcium (CAC) score was obtained and evaluated, as previously reported by Andersen et al. We used the CAC reference value derived from the Multi-Ethnic Study of Atherosclerosis (MESA) to correct our data by age and gender. According to MESA, 20 patients had a CAC score outside the ninetieth percentile for subjects of the same age and gender who were free of cardiovascular disease.
The data are expressed as the mean ± SD or percentages. The CAC score is reported as the median and range. Comparisons among the 2 patient groups and the healthy subjects were assessed by analysis of variance with Bonferroni’s correction. An unpaired sample t test was used to determine the differences between the patient characteristics for the continuous variables. The chi-square test was used to determine the differences between 2 groups of the categorical variables. The data were analyzed using the Statistical Package for Social Sciences, version 16.0 (SPSS, Chicago, Illinois). Two independent observers analyzing myocardial strain were unaware of the treatment status. Ten randomly selected patients were analyzed repeatedly for reproducibility expressed by Cronbach’s α and Bland-Altman analysis. For all statistical comparisons, p ≤0.05 was considered statistically significant.
Results
Both Hodgkin’s lymphoma survivor groups had received a similar radiation dosage ( Table 1 ). No significant differences were found in the demographic characteristics between those who had or had not received anthracycline ( Table 1 ). Both patient groups were comparable with the healthy subjects in terms of age, although the heart rate was greater in the patient groups.
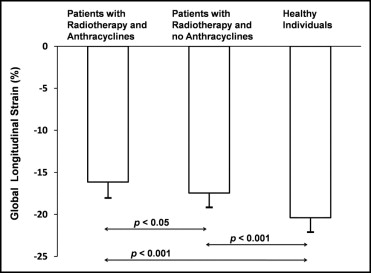
The patients who had received anthracycline and mediastinal radiotherapy had a significantly reduced global longitudinal strain compared to those who had undergone radiotherapy alone or radiotherapy combined with regimens without anthracycline (−16.1 ± 1.9% vs −17.5 ± 1.7%, p <0.05; Figure 1 ). LVEF, however, could not differ between the 2 patient groups (55 ± 8% vs 56 ± 6%, p = 1.0). The healthy participants had better global longitudinal strain (−20.4 ± 1.7%, both p <0.001), circumferential strain (−22.5 ± 2.1%, both p <0.001), and LVEF (62 ± 5%, both p <0.05) compared to either patient group. The circumferential strain was similar among the 2 patient groups (−18.3 ± 3.2% vs −17.8 ± 3.6%, p = 1.0). Figure 2 demonstrates examples of segmental longitudinal strain traces in 2 survivors of Hodgkin’s lymphoma from each patient group and 1 healthy subject.