Left Costovertebral Angle Mass
Jud W. Gurney, MD, FACR
DIFFERENTIAL DIAGNOSIS
Common
Bochdalek Hernia
Aortic Aneurysm
Lipoid Pneumonia
Intralobar Sequestration
Left Lower Lobe Collapse
Less Common
Esophageal Varices
Paraesophageal Hernia
Nerve Sheath Tumors
Sympathetic Ganglion Tumors
Lateral Meningocele
Esophageal Duplication Cyst
Rare but Important
Extramedullary Hematopoiesis
Esophageal Tear
ESSENTIAL INFORMATION
Key Differential Diagnosis Issues
Mnemonic: MASS IN LEFT CV
Meningocele (lateral), aneurysm, sequestration, sympathetic ganglion tumors
Intraabdominal contents (hernias), nerve sheath tumors
Lipoid pneumonia, extramedullary hematopoiesis, foregut malformations (esophageal duplication cyst), trauma (esophageal tear)
Collapse (left lower lobe), varices
Helpful Clues for Common Diagnoses
Bochdalek Hernia
Herniation through posteromedial pleuroperitoneal hiatus
Appearance depends on hernia contents and whether air is present within bowel
In adults: 66% left-sided, 33% right-sided; bilateral in 15%
Aortic Aneurysm
Descending aortic aneurysm may be atherosclerotic, from dissection, mycotic, or traumatic from blunt chest trauma (pseudoaneurysm)
Curvilinear calcification should suggest aneurysm
If left pleural effusion, consider rupture
Lipoid Pneumonia
Aspiration or inhalation of fatty or oily substances: Animal or vegetable oils, mineral oil laxatives, oil-based nose drops, and liquid paraffin
Chronic consolidation with low-attenuation areas (-30 to -150 HU)
Focal consolidation often mass-like
Favors dependent lung segments
Intralobar Sequestration
Sequestration represents nonfunctioning lung tissue separated from normal lung
Receives its blood supply from a systemic artery, lacks normal communication with bronchi
Persistent left-sided (65%) paraspinal mass with history of recurrent pneumonia
Lung may contain solid, fluid, and cystic components (may have air-fluid level)
Systemic artery identification feeding lung is diagnostic
Left Lower Lobe Collapse
Lobe collapses posteriorly, medially, and inferiorly; inferior displacement of hilum
Triangular paraspinal opacification silhouetting medial hemidiaphragm and descending aorta
In adults, must exclude endobronchial obstruction
Helpful Clues for Less Common Diagnoses
Esophageal Varices
Secondary to portal hypertension, most commonly cirrhosis
Dilated, contrast-filled vessels adjacent to esophageal wall
May be unopacified on arterial phase imaging
Associated abnormalities: Cirrhotic liver, splenomegaly
Paraesophageal Hernia
GE junction below diaphragm, gastric fundus intrathoracic
Protrusion usually anterior and lateral to esophagus
Smooth hemispherical retrocardiac mass, usually contains air or air-fluid level
May contain oral contrast
Nerve Sheath Tumors
Neurofibromas or schwannomas
Round posterior mediastinal mass
Dumbbell extension into spinal canal (10%)
Decreased attenuation due to lipid or cystic degeneration
Calcification in 10% of schwannomas
Variable contrast enhancement
Sympathetic Ganglion Tumors
Age related: Neuroblastoma (< 3 years), ganglioneuroblastoma (3-10 years), ganglioneuroma (> 10 years)
Paragangliomas (extraadrenal pheochromocytomas) arise from sympathetic ganglia
Usually arise along sympathetic chain
Elongated vertical posterior mediastinal mass
Often intensely enhance with IV contrast
˜ 85% of neuroblastomas have calcification
Lateral Meningocele
More common in neurofibromatosis type 1, 10% multiple
Right > left
Fluid attenuation; contiguous with thecal sac
Widens neural foramen, scoliosis common
Vertebral bodies often scalloped
Peripheral rim enhancement may occur
Esophageal Duplication Cyst
Foregut malformation: Lung “bud” anomalies
Tubular, oriented vertically along esophagus
Cyst contents usually fluid: Increased attenuation may be due to mucoid, blood, or calcium oxalate contents
Often right-sided
Cyst wall may be thick and calcified
If ulcerated into esophagus or airway, will have air-fluid level
Cyst may contain gastric or pancreatic tissue that may cause hemorrhage, ulceration, or perforation
Helpful Clues for Rare Diagnoses
Extramedullary Hematopoiesis
Associated with chronic anemias, especially sickle cell disease and thalassemia
Multiple lobulated posterior mediastinal masses, vertebral bodies often have prominent trabeculae (from marrow expansion)
Centered on vertebral bodies
Usually contain fat; calcification absent
Will enhance with contrast administration, often inhomogeneous
Esophageal Tear
Etiology: Boerhaave syndrome, instrumentation, blunt chest trauma
Most common location: Left lateral wall of distal esophagus 2-3 cm above gastroesophageal junction
Air in left costovertebral angle (V-sign of Naclerio)
Associated findings: Periesophageal fluid collections, pleural effusion, consolidation or atelectasis of medial basilar segment left lower lobe
May have extravasation of oral contrast
Image Gallery
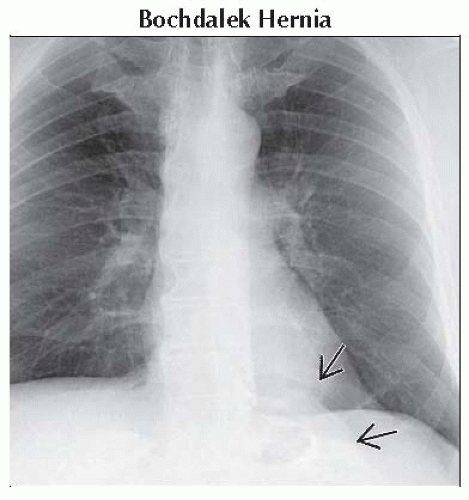 Frontal radiograph shows a well-defined left costovertebral mass  . Mass contains neither air nor calcification. . Mass contains neither air nor calcification. |
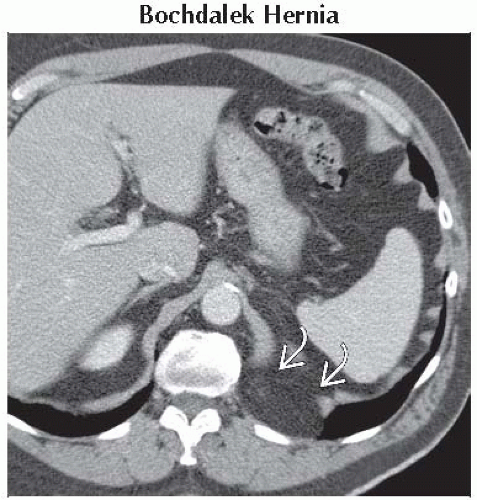 Axial CECT shows localized discontinuity of the hemidiaphragm  with herniation of fat through diaphragmatic defect. with herniation of fat through diaphragmatic defect. |
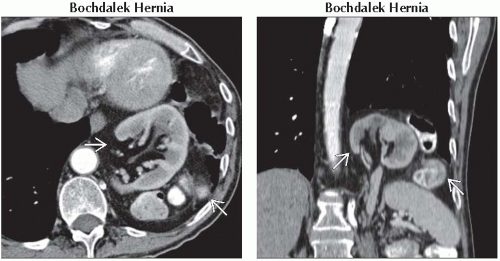 (Left) Axial CECT shows bowel and kidney
 in the left lower hemithorax. Diaphragmatic hernias can be very difficult to visualize on axial images only. (Right) Coronal CECT reconstruction shows herniation of bowel and kidney in the left lower hemithorax. Diaphragmatic hernias can be very difficult to visualize on axial images only. (Right) Coronal CECT reconstruction shows herniation of bowel and kidney  through posteromedial defect. Most Bochdalek hernias contain fat only but may contain kidney or bowel. Coronal and sagittal reconstructions are very useful for identifying diaphragmatic defects. through posteromedial defect. Most Bochdalek hernias contain fat only but may contain kidney or bowel. Coronal and sagittal reconstructions are very useful for identifying diaphragmatic defects.Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|