Figure 13.1
(a, b) Laser resection of small metastases located at the lung periphery is easy and self-explanatory. Using the diode laser system, the bare fiber is grasped with a “penholder,” then lightly touched to the lung tissues. The resection starts by circumscribing the metastasis using a power output of 50–60 W, leaving a 5-mm rim around the metastasis. It is important to compensate for the shrinkage of irradiated tissue to assure that the 5-mm margin is maintained in all directions. Compared with the noncontact resection technique (using the 40-W laser and focusing handpiece), this direct contact technique (using the bare fiber and a 60-W power output) is both threefold faster and nearly smog-free. The noncontact modus also is far more difficult because the surgeon must maintain the fiber at a stable distance from the operative lung, which moves continuously because of the unavoidable movement of the underlying ventilated lung and the beating heart
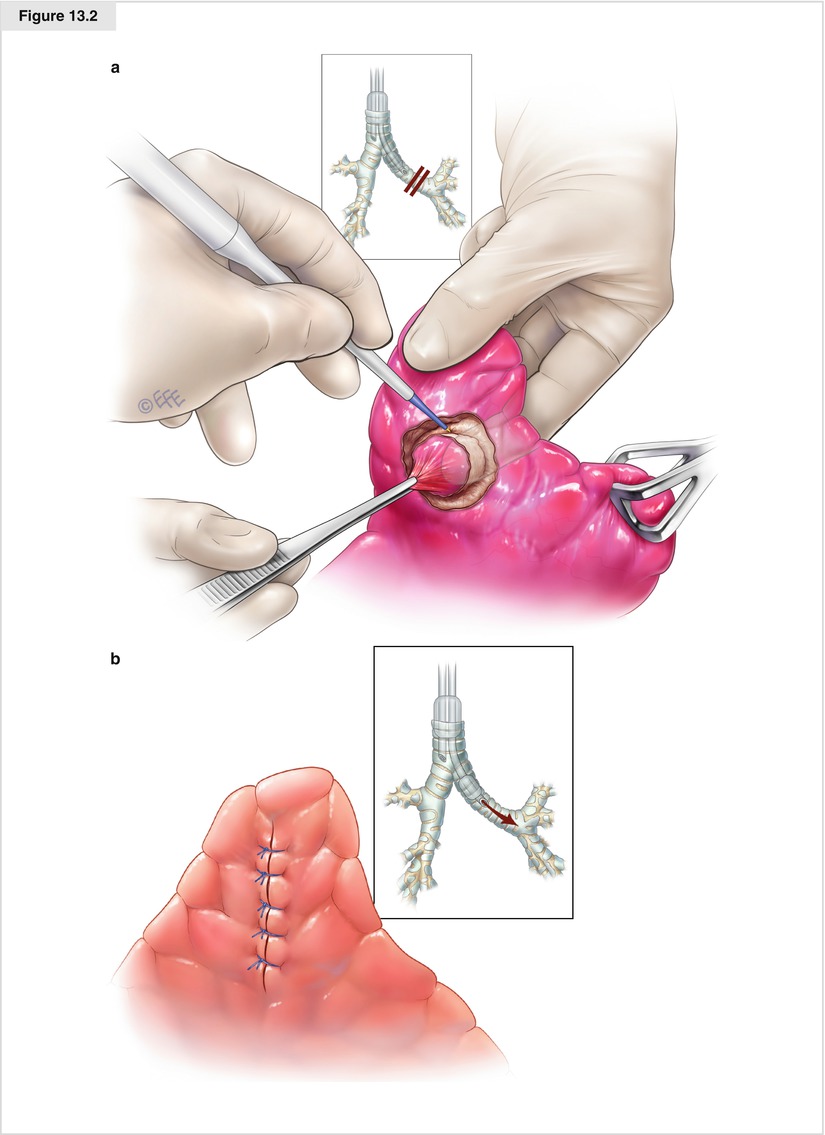
Figure 13.2
(a, b) To resect centrally located and nonvisible metastases in the deflated lung, the lobe is first luxated by graspers. The right-handed surgeon then uses the left hand to precisely locate the metastasis. Next, he or she uses the left index finger to push the metastasis from behind, so it protrudes out against the surface of the lung. A circular cap of overlying lung tissue is then circumferentially resected, and the first assistant retracts it using forceps. By moving and pulling this cap of tissue, the assistant helps the surgeon deepen the laser resection around the metastasis, and ultimately to luxate it so the resection can be completed toward the center of the lobe (much like digging out the rootstock of a tree)
Other Pitfalls
Even experienced thoracic surgeons must undergo a learning curve to become proficient in this open-lung parenchymal resection technique, because it differs in many respects from the closed (stapler or clamp) sublobar resections they are used to performing. However, this extra effort is justified by the remarkable preservation of lung tissue possible using laser resection. With laser, the resection can precisely follow the geometry of the metastasis, whereas clamp or stapler resection must follow the linear structure of the instruments, which produces a significantly greater loss of tissue. Figure 13.1 shows the position of the clamps necessary to assure a 1-cm margin to a metastasis 3.5 cm in diameter, centrally located in the lower lobe. This positioning would produce a tissue loss of 616 cm3 (11 × 14 × 4 cm) from the lung—fully ninefold higher than the loss experienced with photothermal precision laser resection, which is only 64 cm3 (4 × 4 × 4 cm).
Fortunately, the learning curve is shortened by the bloodless nature of laser resection, which aids the surgeon in recognizing the structures dissected so that even when unintended direct contact occurs with a centrally masked metastasis, it is easy to reestablish the 5-mm resection margin around this lesion. It is primarily the dense band of coagulation produced by the 1318 nm laser that enables the surgeon to cut through a complete lobe from the periphery to the central parts without parenchymal bleeding. When a vessel greater than 3 mm in diameter is crossed during laser resection, a suture is usually required to prevent postoperative bleeding. After performing many open lung parenchyma resections, the surgeon will become adept at recognizing structures of this caliber inside or at the lobar hilum, and he or she may suture these vessels prophylactically before they rupture. To suture the vessels and bronchi in the laser resection cavern, absorbable 0000 Vicryl (Ethicon, Somerville, NJ), which has a rough surface favorable for compressing the laser-coagulated tissue, is recommended. In contrast, the flat and stiff suture material usually used to close vessels bears the risk of cutting through this coagulation zone, resulting in delayed postoperative bleeding or bronchopleural fistula. When palpation confirms the close proximity of the central vessels, it is necessary to dissect the vessels (arteries as well as veins) and take them on a loop. The laser resection then resumes from the periphery and proceeds toward the center. When the parenchymal resection reaches the level of the vessels, the vessel is then ligated to assure the high water content for optimal coagulation under blood supply.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


