Ischemic stroke occurring during intercourse in young patients is exceedingly rare. We present 2 cases of young women taking oral contraceptives, each presenting with an ischemic stroke. Transthoracic echocardiography revealed a patent foramen ovale in one patient and an atrial septal defect in the other. The most likely cause of stroke in both patients is embolic. Despite conflicting evidence, young patients presenting with ischemic stroke and found to have a patent foramen ovale or atrial septal defect should be considered for possible device-based closure.
Reports of sexual intercourse provoking ischemic stroke in young patients are exceedingly rare. We present 2 cases of young women taking oral contraceptives presenting with ischemic stroke during intercourse, and both were found to have atrial septal abnormalities.
Case Description
Patient 1
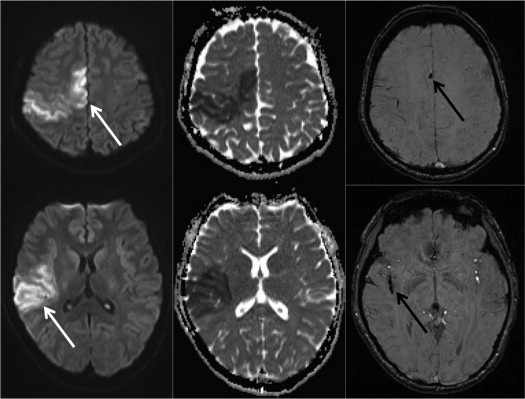
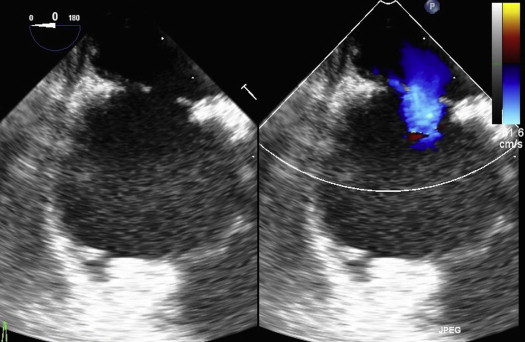
A 25-year-old healthy woman presented to another hospital with acute left-sided weakness and sensory loss occurring during intercourse. Noncontrast computed tomographic scan of the brain was unremarkable. Magnetic resonance imaging of the brain showed diffusion restriction in territories supplied by the right middle and anterior cerebral arteries, consistent with acute ischemia ( Figure 1 ). Physical examination revealed dense left hemiparesis and hemisensory loss as well as a fixed split-second heart sound without murmurs. The computed tomographic angiography finding was negative for carotid dissection, which was further confirmed on black blood magnetic resonance imaging. Transthoracic echocardiography revealed an atrial septal defect (ASD) measuring 1.1 cm with a left-to-right shunt and mild right atrial enlargement, which was confirmed on transesophageal echocardiography ( Figure 2 ). Upper and lower extremity ultrasound study results were negative for deep venous thrombosis. Thrombophilia workup was negative. The patient’s only identifiable risk factor for stroke was oral contraceptive use starting several months before her presentation. Her ASD was closed several months later using a 15-mm Amplatzer Septal Occluder device (St. Jude Medical, Inc, St. Paul, Minnesota). Unfortunately, she had persistent, spastic, left-sided hemiparesis.
Patient 2
A 29-year-old healthy woman presented to our clinic for consideration of patent foramen ovale (PFO) closure. She initially presented to another hospital with sudden-onset right-leg hemiparesis and aphasia immediately after intercourse. In the 3 months before this acute presentation, she had initiated oral contraceptives and experienced several transatlantic flights. Cerebral angiography at the time of presentation showed a filling defect in the middle cerebral artery. Tissue plasminogen activator was administered with complete resolution of her symptoms. A transthoracic echocardiography confirmed a PFO with right-to-left shunting of agitated saline but was otherwise normal. She elected to undergo PFO device closure. Intracardiac echocardiography showed a PFO with a large amount of right-to-left shunting, which was successfully closed with a 25-mm Amplatzer Cribriform Septal Occluder device (St. Jude Medical, Inc).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


