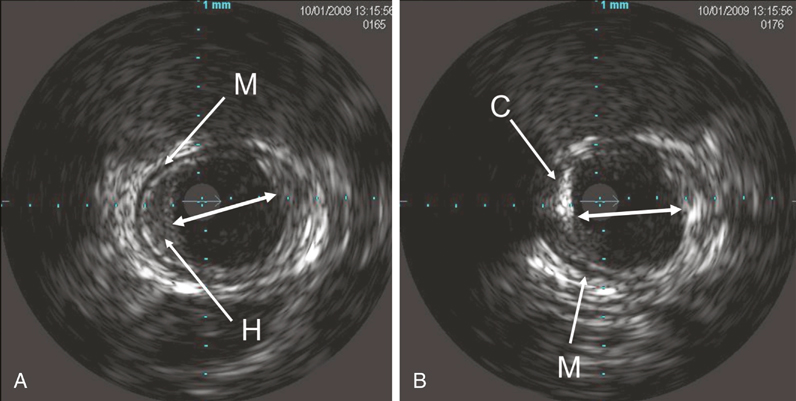
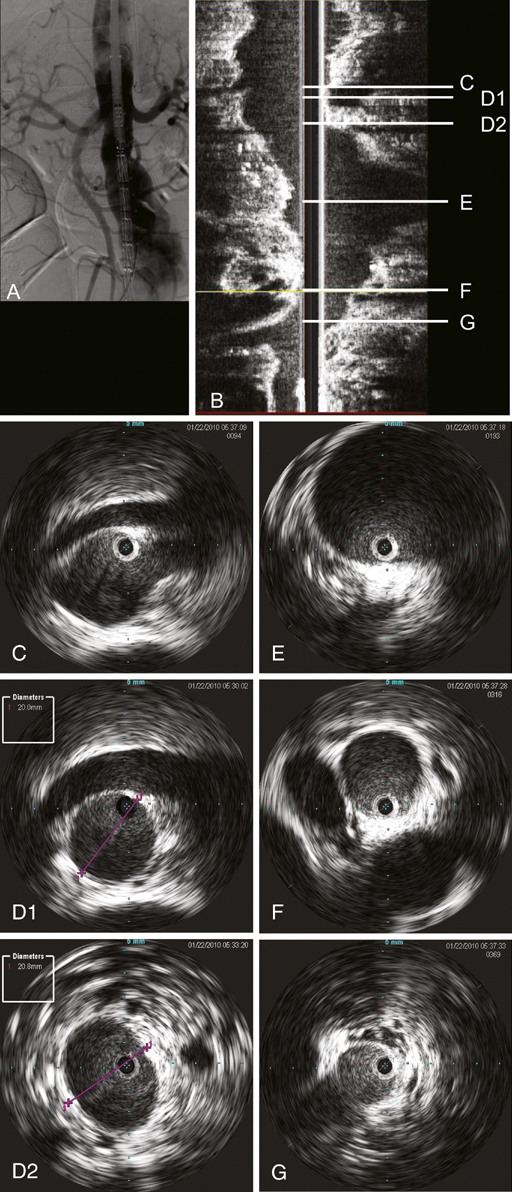
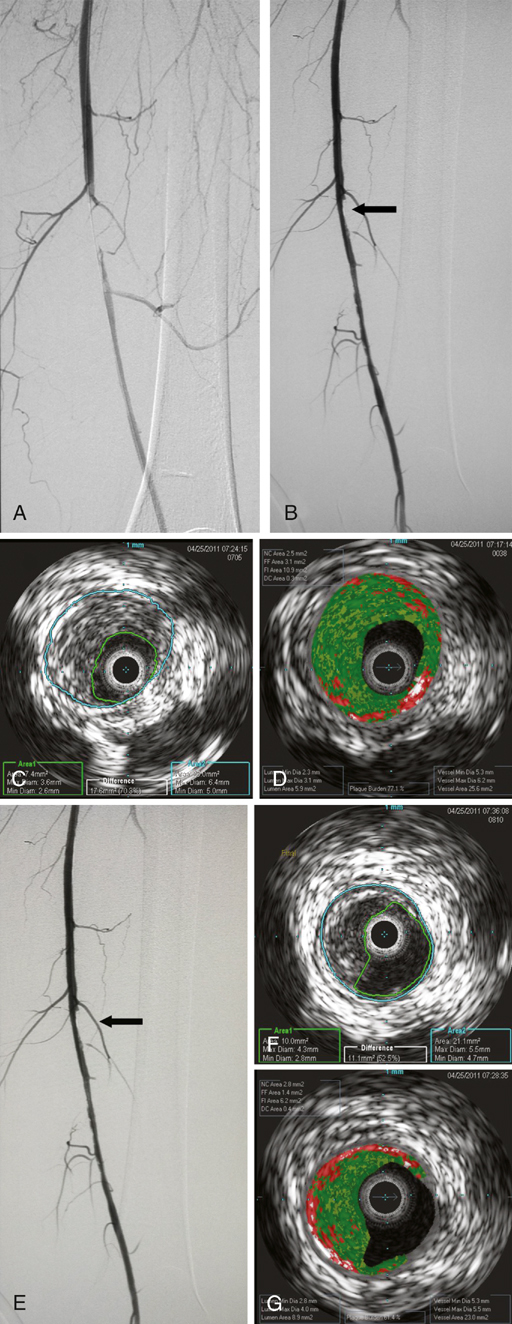
Several studies have reported that IVUS is accurate in determining the luminal and vessel wall morphology of normal or minimally diseased arteries both in vitro and in vivo. In muscular arteries, distinct sonographic layers are visible, with the media appearing as an echolucent layer between the more echodense intima and adventitia. Even small intimal lesions such as flaps or tears are well visualized because of their high fibrous-tissue content and the difference in echoic properties of these structures when compared with surrounding blood. This three-layer appearance is not readily seen in larger vessels, such as the aorta, because of the increased elastin content in the media (Figure 1). Intravascular ultrasound devices are sensitive in differentiating calcified and noncalcified vascular lesions. Because the ultrasound energy is strongly reflected by calcific plaque, it appears as a bright image with dense acoustic shadowing behind it. Gussenhoven and colleagues described four plaque components that can be distinguished using 40 MHz IVUS in vitro: echolucent, which is lipid; soft echoes, fibromuscular tissue, and intimal proliferation, including varying amounts of lipid; bright echoes, collagen-rich fibrous tissue; and bright echoes with acoustic shadowing, calcified tissue (see Figure 1). Advances in image processing and computer technology have resulted in the availability of longitudinal gray-scale IVUS image construction. Longitudinal reconstructions of the IVUS images are obtained by slowly withdrawing the catheter through a vessel. A computer acquires the images, rotates the images 90 degrees, and stacks them to display a longitudinal gray-scale reconstruction. If the pull through is performed with an integrated pullback sled, distances can be measured on the reconstructed image. The current pullback sleds operate at speeds too slow to be useful for peripheral or aortic procedures. For these cases, the investigator can obtain a longitudinal image by pulling the catheter through the vessel by hand, but distances between points cannot be measured. Longitudinal gray-scale IVUS has a unique potential to display vascular pathology, distribution, and tissue characteristics along the length of the vessel, which can be visualized much like an angiogram but with associated wall morphometry (Figure 2). Virtual histology is an imaging option available with the phase-array IVUS catheters. It uses spectral analysis of the radiofrequency ultrasound backscatter signals to identify components of atherosclerotic lesions. The system color codes the four different tissue components: fibrous (green), fibrofatty (light green), dense calcium (white), and necrotic core (red) (Figure 3). The color-coded map helps the investigator understand how the lesion will react to the selected treatment: Will the lesion resist stent deployment or will it be liable to embolization? It is postulated that acute coronary syndromes may be caused by the lipid-rich necrotic core and a rupture of the overlying fibrous cap following angioplasty. This type of plaque differentiation using virtual histology might also play a future role in the selection of carotid stent procedures as well as peripheral vascular interventions (see Figure 3).
Intravascular Ultrasound for Imaging of Diseased Arteries
Intravascular Ultrasound Imaging
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Thoracic Key
Fastest Thoracic Insight Engine
