tubular vascular structures during the final placement of therapeutic devices such as coronary stents.4,5
Table 3.1 Major Differences Between Cardiac Imaging for Dedicated Diagnostic Purposes Versus Image Guidance of Therapeutic Procedures | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
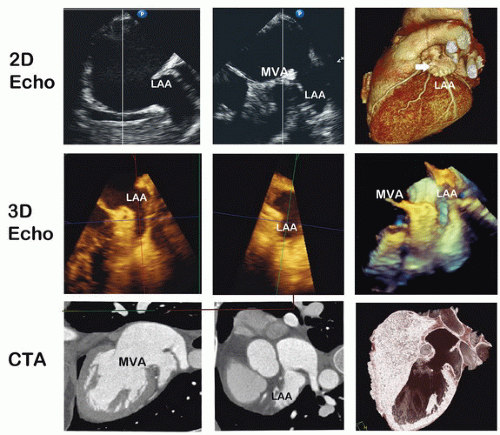 Figure 3.1 Comparison of imaging modalities characterizing the left atrial appendage structure. Biplane echocardiography is shown in the top row with the exception of the far-right image which is a surfacerendered 3D volumetric CTA display. Note the double lobes on the 3D image not appreciated on the 2 orthogonal plane echocardiographic images. The second row is 3D echocardiographic images showing the greater detail of the left atrial structure in MPR and 3D display modes. CTA 2D orthogonal views show both the internal chamber and the atrial tissue. The last image shows the threshold inversion method again giving the 3D appearance of the target structure. |
not only be able to show gray scales but also the color used to represent “depth” in 3D ultrasound images. Initially, the monitor bank was expanded with dedicated monitors for different image-based information. More recently the large single screen technology has emerged. This technology provides maximal flexibility in displaying images and other information needed during the procedure.12 The potential of displaying medical images in a holographic format is a new exciting development that may be initially tested in the cardiac catheterization environment and studied for its impact on the performance of interventions optimally performed with 3D visualization.
Table 3.2 Overview of Real-Time Imaging Modalities to Guide the Performance of Diagnostic and Interventional Tasks in The Cardiac Catheterization Laboratory | ||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
expansion of the team of physicians and staff. With complex SHD interventions it has become essential that a colleague expert in ultrasound, including 3D transesophageal echocardiography (TEE), be part of the interventional team.
Table 3.3 Examples of Study Designs to Determine Relative Merits of Different Image Guidance Strategies | |||||||||
|---|---|---|---|---|---|---|---|---|---|
|
or stenotic cardiac valves18, 19, 20, 21 utilizing the emergence of supportive image guidance. As more structural interventions are adopted, proceduralists are required to become adept at utilizing imaging technology that not only identifies vascular lumen or gross anatomy, but also images soft-tissue and adjacent structures. Future structural interventions hinge on the integration of imaging to navigate cardiac chambers, target different structures, and deploy a variety of therapeutic devices. Current methods such as x-ray fluoroscopy, 2D echocardiography, 3D echocardiography (3DE), cardiac MR, and cardiac CT have developed independently and merged into important adjuncts that enable the execution of complex structural interventions.8,22, 23, 24, 25 In general, there are common elements to the process of executing structural interventions; however, individual procedures emphasize particular elements. The common elements include preprocedural planning, targeting, detection/positioning and tracking, mechanical biofeedback/ eye-hand coordination, precise repositioning and alignment, navigation, 3D localization, deployment surveillance, and postprocedure inspection (Figure 3.2). These functions are discussed further in subsequent parts of the chapter and in the case-specific tasks.
Table 3.4 Assessment of Image Guidance Technology | ||||||
|---|---|---|---|---|---|---|
|
more user-friendly compared to prior platforms.34 Real-time 3D transthoracic echocardiography (RT3D TTE) has been clinically implemented to improve endomyocardial biopsy accuracy35 and off-pump mitral valve (MV) edge-to-edge repair in a pig model.36 This was expanded to successful percutaneous ASD closure.37 The development of real-time 3D imaging with both transthoracic (3D TTE) and transesophageal echocardiography (3D TEE) integrates moving structures with definition of depth in wide field of views providing superior structure resolution. This allows definition of cardiac defects, chambers, and valves while directly and simultaneously monitoring movements of interventional devices.
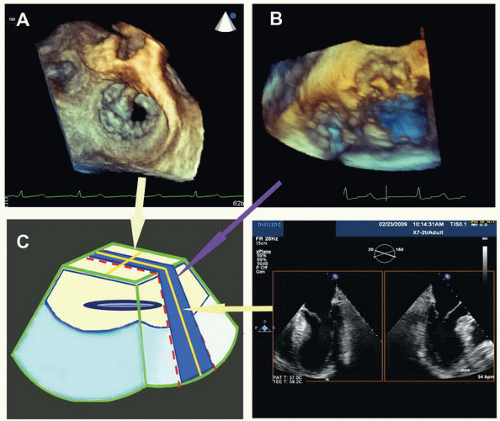 Figure 3.2 Graphic display of the volume images is shown by the three different 3D echocardiographic methods. RT3D TEE focused method is shown in panel A, which is at a focused depth that magnified 3D dataset (crème color). Shown in panel B is the narrow sector RT3D “live” method (blue color); note the larger FOV but, with less depth or thickness. Panel C, the steerable biplane technique shows the orthogonal nature of the planes (yellow lines). |
moving cardiac structures. This is a summation of four adjacent wedge-shaped volumetric datasets acquired sequentially over four cardiac cycles, with subsequent fusion into a single large echosector (Figure 3.3C).39 The dataset may be viewed offline in operator-defined cropped planes in any axis and orientation, offering several visual vantage points ideal for preprocedural planning.
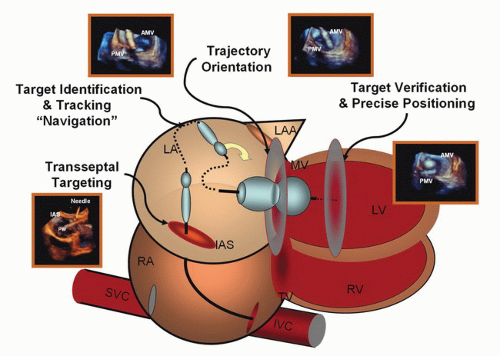 Figure 3.3 Steps for image guidance are shown. Using a mitral valve balloon valvuloplasty as an example, each key stage is shown: first, transseptal puncture; second, identification of the target; positioning and definition of trajectory; and target verification and precision adjustment. Each step is important for preplanning and procedural guidance. |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


