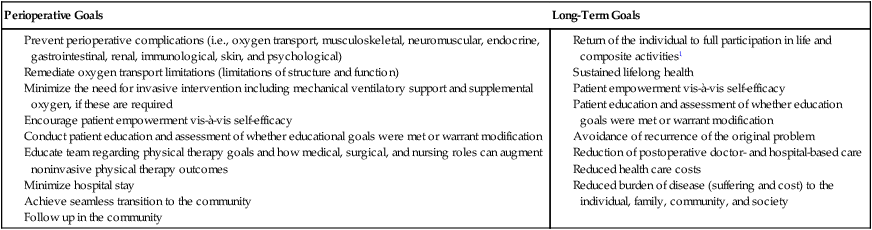
The decision as to whether and to what extent physical therapy is indicated is based on the individual’s need rather than strictly on his or her condition. The patient’s condition is one factor that can determine perioperative risk, operative course, and long-term outcomes. Factors other than the primary indication for surgery, however, can have a more important effect on perioperative course and outcomes. Because of this, the preoperative assessment determines who requires physical therapy management and who does not. Physical therapy prevents complications and addresses oxygen transport threats and deficits. In the long term, physical therapy helps ensure that the individual returns to the highest level of living and regains or surpasses premorbid presurgical functional status. In cases in which the underlying condition can recur, a prime physical therapy objective is to minimize this possibility. Surgical outcomes, based on the physical therapy perspective within the International Classification of Functioning, Disability and Health,1 are shown in Box 30-1. Box 30-1 Surgical Outcomes and their Components Related to Physical Therapy The purpose of this chapter is to review the identification of surgical risk in a given individual and the management of patients with cardiovascular and pulmonary risk factors and dysfunction secondary to acute surgical conditions. Surgery today has become more extreme in two ways. First, minimally invasive surgery has shortened the operative period, hastened discharge, and reduced risk.2 Second, with advances in instrumentation, monitoring, and anesthesia, more invasive, prolonged, and risky surgery is being performed with improved chances of survival. The cardiovascular and pulmonary effects of anesthesia and surgery are described. The two types of surgery that have the greatest impact on cardiovascular and pulmonary function, namely thoracic and cardiovascular surgery, are highlighted. These surgeries are particularly invasive and lengthy, often require heavy and prolonged anesthesia and sedation, are typically performed on older people whose health status may be poor, and are generally associated with increased risk. Thus they warrant intensive perioperative physical therapy. Patients are assessed with respect to their presurgical and surgical hemodynamic and oxygen transport status to establish oxygen transport capacity and the degree to which increased metabolic demands associated with the perisurgical conditions as well as interventions can be met. In particular, cardiac output and oxygen delivery (DO2) will increase to compensate for these increased metabolic demands. Increased metabolic demands, however, are dependent on age, severity of illness, type of surgery, comorbidity, and complications.3 Furthermore, people who are overweight or obese, a common lifestyle-related condition, are more likely to require surgery. Obesity can reduce arterial oxygen tensions and the compliance of the respiratory system irrespective of the tidal volume or respiratory rate.4 A detailed analysis of these factors can identify risks, expedite early intervention such as mobilization, and increase survival. The four categories of factors that threaten or impair oxygen transport are described in Chapter 17. These factors include the underlying pathology, restricted mobility and recumbency, extrinsic factors related to the patient’s care, and intrinsic factors related to the patient. This chapter examines in detail the effects of surgery, including the effects of anesthesia and other medications on oxygen transport as well as the impact of the underlying condition, restricted mobility and recumbency, and factors associated with the patient on an individual’s status postoperatively. These are described in a format to facilitate assessment and ongoing evaluation. Treatment principles are presented. These are not intended, however, to be a treatment prescription for a particular patient. The effects of anesthesia and surgery must be considered in addition to the underlying pathology and the effects of restricted mobility, body position, and intrinsic and extrinsic factors (see Chapter 17). All these factors must be considered and integrated in prescribing treatment and defining the specific parameters of the prescription. Such integration is essential for treatment to be targeted to the underlying problems and to be maximally effective. Factors that place a patient at risk can contribute to perioperative cardiovascular and pulmonary dysfunction if preventive strategies fail (Box 30-2). Cardiovascular and pulmonary complications are the major cause of perioperative morbidity and mortality, particularly in patients undergoing thoracic or cardiovascular surgery.5 The physical therapist must establish the risk factors based on premorbid health assessment including age, smoking habits, nutrition, weight, regular physical activity and fitness, sleep, and stress, as well as cardiac dysfunction, lung dysfunction, musculoskeletal dysfunction, neuromuscular dysfunction, and endocrine dysfunction—in particular, type 2 diabetes mellitus.6 Box 30-2 Surgical Factors that Contribute to Perioperative Cardiopulmonary Risk and Dysfunction Physical therapy has a role in preparing patients for surgery some weeks in advance—a service that is not being fully exploited in health care. Maximizing a patient’s health will lead to fewer complications, will shorten hospital stay, and will hasten recovery and return to full participation in daily life. Interventions can include health education, including initiating or supporting smoking cessation. Smoking cessation or smoking reduction by at least 50% has been shown to improve the outcomes after hip and knee replacements.7 Comparable benefits could be expected for other types of surgery, particularly cardiovascular and thoracic procedures. Optimizing nutrition and prescribing an exercise program, even if modified because of the patient’s underlying condition, can augment oxygen transport. Thus, when oxygen transport is unavoidably compromised by anesthesia and surgery, the patient has greater reserve capacity. People who are overweight and obese have direct, serious weight-related morbidity including hypertension, type 2 diabetes mellitus, lipid-related heart conditions, and sleep apnea. In addition, people who require joint replacement surgery because of arthropathy secondary to irreversible joint damage are more likely to be overweight.8 Thus, overweight and obesity constitute major complications during surgery and recovery. Given their prevalence, overweight and obesity warrant being addressed by physical therapists in every patient, whether surgical or medical (see Chapters 1 and 6). Furthermore, body mass index as well as weight-to-hip ratio and age have been reported to be significant predictors for type 2 diabetes mellitus and hypertension, which further complicates the clinical presentation and management of surgical patients who are overweight or obese.9 Early surgery for hip fracture in older adults has not been shown unequivocally to result in improved outcomes—that is, reduced complications (pneumonia and bed sores), earlier recovery, and reduced mortality.10 It is likely that clinically some patients may benefit whereas others may benefit from some delay. Irrespective, the outcomes of physical therapy will be enhanced in either situation if instituted in a timely manner. Studies are needed to establish the degree to which physical therapy including lifestyle behavior change (weight loss in particular) may avert surgery all together, or appropriately delay it. In some patients, early surgery may be preferable. In this case, some finite period of time in which a course of physical therapy could be instituted prior to surgery, could augment surgical outcomes. Anesthesia results in depression of breathing. Thoracic respiratory excursion is reduced. The tone and pattern of contraction of the respiratory muscles, particularly the diaphragm and the intercostal muscles, change, which contributes to many secondary cardiovascular and pulmonary effects observed after surgery. The loss of end-expiratory diaphragmatic tone causes the diaphragm to ascend into the chest by 2 cm during anesthesia with or without paralysis.11 Reductions in functional residual capacity (FRC) are correlated with this change and with altered chest wall configuration and increased thoracic blood volume.12,13 One of the most pervasive and predictable clinical effects observed in the postoperative period is alveolar collapse. Total lung capacity, FRC, and residual volume are decreased. The FRC is reduced in the supine position compared with the erect sitting position14,15 and is further reduced with the induction of anesthesia. Anesthesia, however, fails to reduce FRC in the sitting position. The consequences of reduced FRC with anesthesia and surgery have major implications for postoperative complications and the course of recovery. Airway closure occurs with anesthesia, and this likely contributes to intrapulmonary shunting. Compression atelectasis of the dependent (lowermost) lung fields occurs during surgery.16 In addition, compression atelectasis occurs when lung tissue and surrounding structures are being physically manipulated by the surgeon. Although reduced airway caliber in areas of low lung volume can be offset by the airway-dilating effect of many inhaled anesthetics, airway resistance is increased by obstruction of the breathing circuits, valves, and tracheal tubes. The airways may also be obstructed with foreign matter such as blood and secretions, or from bronchospasm caused by irritation. Because of the decrease in FRC, lung compliance is decreased and the work of breathing is increased. Hypoxemia secondary to transpulmonary shunting is usually maximal within 72 hours after surgery and may not be completely resolved for several days. Persistent reduction in FRC after surgery delays the restoration of the normal alveolar-arterial oxygen gradient. Anesthesia and tissue dissection contribute to major changes in lung volume, mechanics, and gas exchange. The extent and duration of these changes increase with the magnitude of the operative procedure and degree of anesthesia required. Tissue oxygenation can be threatened during the intraoperative period, and the relationship between oxygen consumption (VO2) and delivery (DO2) compromised.17 Mismatch between VO2 and DO2 is associated with a complicated clinical course and prolonged intensive care unit stay in the absence of conventional indicators such as low ejection fraction and longer cardiovascular and pulmonary bypass time.18 Oxygen extraction increases to compensate for reduced DO2. Early optimization of the ratio of VO2 and DO2 is indicated to reduce perioperative morbidity and mortality. After surgery the normal pattern of breathing is disrupted. Shallow, monotonous tidal ventilation without normal occasional, spontaneous deep breaths causes alveolar collapse within an hour.15 Unless resolved within a few hours, atelectasis becomes increasingly resistant to reinflation. This complication is exacerbated in patients receiving narcotics. After surgery the patient is detained in the recovery room until vital signs have stabilized, there is no apparent internal or external bleeding, and the patient is responding to his or her name. Patients recovering from minor surgery are usually transferred to a ward once discharged from the recovery room. A patient is transferred to the intensive care unit after surgery if complications arose during surgery, if the patient cannot be readily stabilized and requires close monitoring, or if the patient had more serious surgery such as cranial, cardiovascular thoracic, or emergency surgery such as that resulting from multiple trauma (see Chapter 35). Common pharmacological agents prescribed for patients perioperatively are described in Chapter 45. Physical therapists need a thorough knowledge of these when managing the surgical patient so management can be optimized. Several factors are particularly important in managing surgical patients because these factors can affect the patients’ sensitivity to narcotic analgesics such as morphine.19,20 There is considerable intersubject response variability to these agents. Older patients, for example, can be expected to be more sensitive to narcotics. Diverse multisystem pathology has a marked effect on the degradation, absorption, biotransformation, and excretion of morphine. Exaggerated effects of morphine have been reported when administered in conjunction with other agents such as other narcotic analgesics, phenothiazines, tranquilizers, or sedative-hypnotics; in addition, such exaggerated effects have been reported in patients with respiratory depression, hypotension, and sedation and in patients who are unconscious. Situations in which exaggerated drug effects have been reported are commonly encountered in the intensive care setting and can result in unpredictable responses. Finally, the physical dependence and abuse potential of these agents cannot be ignored. The administration of narcotics has important implications for physical therapy. These powerful analgesics are often the medications of choice for major pain relief and comfort. Their secondary effects, however, which include reduced arousal and monotonous tidal ventilation, are primary physical therapy concerns. Narcotics interfere with a patient’s ability to cooperate with treatment. If narcotics impair the patient’s ability to participate in treatment, analgesia with a less systemic effect is indicated. Patient-controlled analgesia (PCA) is an effective means of having the patient regulate the amount of analgesia he or she is receiving.21 Patients have been reported to administer less medication to themselves than nurses assessing their analgesia needs. Intravenous administration prolongs the peak-effect time of analgesics and therefore helps the patient tolerate longer, more intense treatments. Oversedation must be avoided if the patient is to derive maximal benefit from cardiovascular and pulmonary physical therapy treatments.
Individuals with Acute Surgical Conditions
 The patient’s complete return to full participation in life and the capacity to perform its requisite activities
The patient’s complete return to full participation in life and the capacity to perform its requisite activities
 Avoidance of recurrence of the problem for which the individual’s surgery was indicated
Avoidance of recurrence of the problem for which the individual’s surgery was indicated
 Reduced subsequent doctor- and hospital-based care and need for medication
Reduced subsequent doctor- and hospital-based care and need for medication
Perioperative Course
Surgery and Its Cardiovascular and Pulmonary Consequences
 Anesthetics (general, with or without intubation, or regional) and sedation and reduced arousal
Anesthetics (general, with or without intubation, or regional) and sedation and reduced arousal
 Muscle-relaxant agents and neuromuscular blockade
Muscle-relaxant agents and neuromuscular blockade
 Supplemental oxygen and humidification
Supplemental oxygen and humidification
 Duration of surgery and static body positioning
Duration of surgery and static body positioning
 Use of the cardiopulmonary bypass machine (CBM)
Use of the cardiopulmonary bypass machine (CBM)
 Use of the extracorporeal membrane exchanger (ECMO)
Use of the extracorporeal membrane exchanger (ECMO)
 Chest tube placement and number
Chest tube placement and number
 Perioperative anxiety, discomfort, and pain
Perioperative anxiety, discomfort, and pain
 Perioperative pain control management
Perioperative pain control management
 Perioperative fluid balance management
Perioperative fluid balance management
Anesthesia and Supplemental Oxygen
Immediate Postoperative Period
Pharmacological Considerations
 Have nonpharmacological means of analgesia been exploited?
Have nonpharmacological means of analgesia been exploited?
 If pharmacological analgesia is indicated, could analgesics other than narcotics be used?
If pharmacological analgesia is indicated, could analgesics other than narcotics be used?
Individuals with Acute Surgical Conditions















