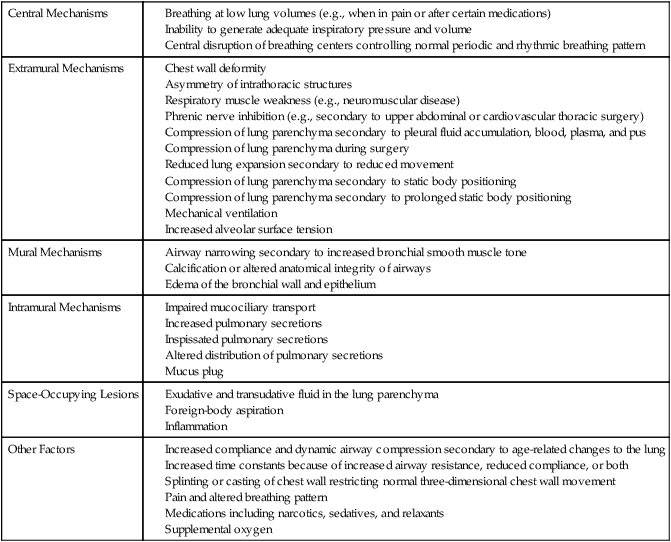
This chapter describes the physical therapy management of individuals with primary, acute dysfunction of the cardiovascular and pulmonary systems. Such dysfunction may limit participation in life and its related activities in the short- or long-term. Further, such dysfunction can constitute life threat in the absence of limitations to life participation and quality of life (e.g., hypertension and dysrhythmias). Management principles for people with several types of common acute medical conditions are described. Although medical conditions are usually classified as either primary pulmonary disease or primary cardiovascular disease, the heart and lungs work synergistically to effect gas exchange and cardiac output and in series with the peripheral vascular circulation to effect tissue perfusion.1,2 Thus impairment of one organ system invariably has implications for the function of the other. Threat to or impairment of oxygen transport has implications for all other organ systems; thus a multisystem approach is essential for overall management (see Chapters 1 and 5). The primary, acute pulmonary conditions that are presented in this chapter include atelectasis, pneumonia, bronchitis, bronchiolitis, acute exacerbations of chronic airflow limitation, asthma, cystic fibrosis, interstitial pulmonary fibrosis, and tuberculosis. For further epidemiological and pathophysiological detail on these conditions, refer to Mason and colleagues (2010)3 and West4 (2007). The primary, acute cardiovascular conditions presented include hypertension, medically stable angina, and uncomplicated myocardial infarction. For further details on these conditions, refer to Sokolow and Cheitlin5 (2004), Fauci and colleagues6 (2008), and Woods and colleagues7 (2009). The pathophysiology underlying the medical management of each condition extends the pathophysiology content of Chapter 5 and, in turn, provides a basis for each condition’s physical therapy management. The management principles presented are not intended to serve as treatment prescriptions for any particular patient. The treatment priorities presented are based on the underlying pathology, as well as the potential complexity of its manifestation for a patient. Without discussion of a specific patient and knowledge of other clinically relevant factors (i.e., the effects of restricted mobility, recumbency, and the effects of extrinsic and intrinsic factors on the patient’s presentation including sociocultural context; see Chapter 17); however, the specific parameters of the treatment prescription cannot be completely established. Integration of patient-specific information is essential for treatment to be specific and maximally effective. Chapter 31 extends the principles involved with the management of many of the acute medical conditions described in this chapter, detailing their subacute and chronic stages. Essential hypertension, the “silent killer” (of unknown etiology), is the most common type of hypertension (90% of all reported cases). Although salt sensitivity has been implicated in hypertension in African Americans and increased rennin production in the Hispanic population,8 salt consumption is a serious health concern in the North American population. Widespread campaigns are being aimed at reducing salt consumption in the pediatric as well as adult population.9 Reducing consumption by one-third is estimated to reduce the prevalence of hypertension substantially. Generally, hypertension is classified as mild, moderate, or severe. It is generally managed pharmacologically with vasodilators (i.e., afterload reducers), diuretics (i.e., volume reducers), and beta-blocking agents (i.e., inotropic agents). Despite a primarily pharmacological orientation to the management of hypertension, a high proportion of individuals with hypertension still have high blood pressure and are at increased risk for its deadly complications. Hypertension is a significant health care concern in that the condition is frequently associated with heart disease, stroke, and renal dysfunction and failure.10 Thus its consequences can be dire. As described in Chapter 1, hypertension often occurs in the presence of obesity and diabetes, which complicates the clinical picture further. 1. To what degree does pharmacological intervention appear warranted, given the patient’s severity of hypertension and overall clinical picture? 2. To what degree could the hypertension be managed with nonpharmacological interventions? 3. To what degree could pharmacological and nonpharmacological interventions be used concurrently? What type of schedule might be anticipated to wean the patient off medication with time or at least minimize it? Physical therapists treat patients with hypertension as a primary or secondary diagnosis. If it is a secondary diagnosis, it is important that the diagnosis is not overlooked. What the physical therapist can do for the hypertension may be clinically more significant than management of the primary diagnosis for which the patient is referred. As with many other lifestyle-related conditions, antihypertensive medication may be perceived by the patient as addressing the problem, whereas in many instances, it only addresses the effect. Lifestyle changes are necessary to normalize blood pressure with the goal of eliminating the need for blood pressure medication.11 Exercise therapy can be an effective intervention for the management of hypertension with the primary goal of eliminating the need for medication.12 Secondarily, physical therapy with a focus on exercise and health education, including smoking cessation and basic nutritional counseling, is aimed at reducing the need for medication or its potency. The foundation of management in a patient with hypertension is a lifestyle review and recommendations in consultation with the patient. Recommendations include nutrition, weight control, exercise, smoking cessation, and stress management.13 Medical management may include beta blockers and diuretics to reduce plasma volume or other antihypertensive medication. A prescription of regular aerobic exercise may control hypertension.14 The prescription is based on a consideration of the patient’s coexistent problems and general health status. If obesity is a concurrent problem, an exercise program is prescribed to address both concerns. A patient who is being managed acutely with high blood pressure may benefit from relaxation strategies, breathing control, and stress management. Further, complementary therapies, as described in Chapter 27 may have an important role. For noninvasive physical therapy management of hypertension, see Chapter 31. The management of patients with ischemic heart disease who are hemodynamically unstable and require intensive monitoring to assess and to monitor physical therapy treatment is described in Chapter 34. This section addresses management of the patient with a cardiac medical condition who is stable and uncomplicated. Physical therapists must be knowledgeable and proficient in management of the patient with cardiac conditions because these patients are referred with cardiac disease as a primary or secondary problem. With respect to heart disease being a secondary diagnosis, patients often come to the physical therapist for the management of an orthopedic complaint with a history of angina, frank myocardial infarction, or hypertension. The principles for physical therapy in management of patients with acute ischemic heart disease are presented within the principles of phase I cardiac rehabilitation (Table 29-1). Because physical therapy invariably involves physically stressing a patient either with therapeutic exercise or with the application of a therapeutic modality, the physical therapist must address the following questions when managing a patient with ischemic heart disease and its risk factors: Table 29-1 Phase I of Cardiac and Pulmonary Rehabilitation (Inpatient, <7 to 10 days)* *Phases II, III, and IV are related to subacute and chronic care (see Chapter 31). Modified from Piotrowicz R, Wolszakiewicz J: Cardiac rehabilitation following myocardial infarction. Cardiology Journal 15:481–487, 2008. 1. Does the patient’s cardiac status preclude treatment? Why? 2. Is additional information about the patient necessary before physical therapy assessment and treatment? What information? 3. How should treatment be modified? Why? 4. Is the patient using antianginal medication appropriately? Is the prescription current? Does the patient have the antianginal medication present at all times? 5. Are there other medications that may influence the patient’s cardiovascular and pulmonary status and response to treatment? What are they? How might the patient’s responses to treatment, particularly exercise, be affected? 6. What physiological parameters should be monitored before, during, and after treatment? 7. What is the patient’s knowledge about his or her condition? Can the patient clearly identify what triggers the angina and what makes it worse and better? What lifestyle changes have been made? What should be reinforced and what education is necessary? Individuals prone to angina may exhibit symptoms in certain body positions.15,16 Usually, this reflects an increased workload and increased work of the heart. Recumbent positions increase the mechanical work of the heart by increasing central blood volume.17 These patients are not encouraged to lie flat. Instead, the head of bed is elevated 10 to 15 degrees. Side-lying positions, particularly left side-lying, increase the work of the heart by compressing the heart and impeding ventricular filling and ejection. Patients with impaired oxygen transport and without prior cardiac disease may exhibit myocardial stress and ischemia in these body positions. Thus patients with impaired or threatened oxygenation must be monitored closely, particularly during turning and activities in which oxygen demand is increased—at these times, oxygen delivery must be increased correspondingly. The use of medication to minimize the risk for angina and ischemic heart disease warrants review. The need for statins, commonly prescribed lipid-lowering medications, can be reduced through optimal lifestyle choices in many patients. One inherent danger of such a drug, however, in addition to its well documented side effects, is that patients may become complacent, believing that the drug will offset the need to make necessary lifestyle changes. More important, lifestyle changes largely address the cause of the problem, whereas medication such as statins only address an effect. The principles of the physical therapy management of patients with stabilized angina include health education, risk factor reduction, and a long-term health program (see Chapters 24 and 31). Myocardial infarction, commonly referred to as a heart attack, refers to insufficient myocardial perfusion resulting in a macroscopic area of damage and necrosis of the heart. Infarction results most frequently from narrowing and occlusion of the coronary blood vessels secondary to atherosclerosis. Other causes include occlusion secondary to a thrombus or embolus, reduced blood pressure, or coronary vasospasm. Angina, or ischemic chest pain, often precedes or accompanies a myocardial infarction. Infarctions vary in severity from being silent (i.e., having no characteristic signs and symptoms and thus going undetected) to being fatal. Most infarctions, when detected, require some hospitalization and monitoring to ensure that the infarction is not evolving further and that the patient is medically stable and in no danger. Chapter 34 describes the management of patients with complicated myocardial dysfunction who are admitted to a coronary care unit. This section focuses on the patient with mild heart disease, the patient with cardiac dysfunction who is discharged from hospital, the patient who has a history of ischemic heart disease, and the patient who is hospitalized for a condition other than heart disease but develops and is being managed for myocardial ischemia. Judicious movement and body positioning are essential elements in the management of the patient with myocardial infarction.18 Because these interventions can place significant demands on cardiovascular and pulmonary function and oxygen transport, they must be prescribed specifically by physical therapists with considerable knowledge and expertise in the area. Table 29-1 shows the primary components of care in the acute phase of management (phase I of cardiac rehabilitation). Physical therapy constitutes a prime hemodynamic stress secondary to exercise and gravitational stress secondary to mobilization/exercise and body position changes. Thus it is essential to establish the adequacy of the patient’s cardiovascular and pulmonary system to effect oxygen transport during and between treatments. The optimal treatment prescription is based on the patient’s overall signs and symptoms of coronary insufficiency and hemodynamic instability. The physical therapist must be knowledgeable in detecting inadequate myocardial tissue perfusion and in reducing and preventing myocardial tissue damage. In addition, acute or chronic impaired heart pump function leads to reduced cardiac output and systemic tissue perfusion. Clinical manifestations include reduced mentation, reduced renal function, fatigue, malaise, and moist, cool, and cyanotic skin. When selecting body positions for the patient with a myocardial infarction, the therapist selects those that will minimize the work of breathing and of the heart.19 Significant central fluid shifts are minimized by encouraging the upright position as much as possible to reduce the work of the heart20 and by raising the head of the bed 10 to 15 degrees when the patient is recumbent. Patients with elevated intracardiac pressures are less susceptible to orthostatism (see Chapter 20). Relaxation is central in the management of the cardiac patient who is prone to being anxious and apprehensive. Furthermore, such patients have a high prevalence of sleep-disordered breathing,21 so a sleep assessment is warranted. Relaxation interventions that can be suggested include autogenic relaxation, progressive relaxation, Benson’s relaxation response procedures, biofeedback, and meditation. Also, the patient needs to identify and minimize stress triggers and effective, individual-specific, nonpharmacological relaxants. Relaxation training with or without pharmacological support can be integrated into treatment.7 Patients with ischemic heart disease are often apprehensive and anxious about the intensity of physical activity they can undertake. Thus performing physical activity and exercise while monitored and under the supervision of a physical therapist is often reassuring and gives the patient confidence to perform activity when unsupervised. Optimal lifestyle habits and a lifelong health plan are central to maximizing recovery and improving an individual’s long-term prognosis. Good nutrition and hydration, good sleep habits, stress management, smoking cessation, and regular physical exercise are all salient to comprehensive physical therapy management (see Chapters 24 and 31). As in the management of patients with other lifestyle-related conditions, the physical therapist needs to reinforce public health policy and health promotion guidelines regarding healthy lifestyle choices, including avoidance of inactivity and regular physical activity.22 Atelectasis refers to partial collapse of lung parenchyma. The pathophysiological mechanisms contributing to atelectasis are multiple (Table 29-2). These mechanisms include physical compression of the lung tissue (e.g., resulting from increased pleural fluid, pus, pneumothorax, compression during thoracic surgery, or adjacent areas of lung collapse) or obstruction of an airway (e.g., due to secretions or tumor) with subsequent reabsorption of oxygen from the trapped air by the pulmonary capillaries resulting in a collapse of the lung tissue distal to the obstruction (i.e., reabsorption atelectasis). Table 29-2 Pathophysiological Mechanisms Contributing to Atelectasis Because it can develop instantaneously when respiratory mechanics are disrupted, microatelectasis should be anticipated and prevented. Those factors that contribute to atelectasis for a given patient are countered accordingly with aggressive prophylactic management. Many of the causes of atelectasis outlined in Table 29-2 can be readily reversed. The assessment includes a detailed analysis of the underlying cause(s) and mechanism(s) so that these can be addressed directly for a given patient. Atelectasis is always treated aggressively because it has the potential to worsen, develop into a severe clinical manifestation, and lead to pneumonia. In turn, overwhelming pneumonia can precipitate acute respiratory distress syndrome (Chapter 36), which is associated with considerably poorer outcomes. Based on long-standing physiological evidence, treatment continues to be primarily directed at reversing the underlying contributing mechanisms whenever possible. For example, atelectasis resulting from restricted mobility is remediated with mobilization. Atelectasis resulting from prolonged static positioning and monotonous tidal ventilation is managed with mobilization, manipulating body position to increase alveolar volume of the atelectatic area, manipulating body position to optimize alveolar ventilation, or some combination of these interventions. Atelectasis arising from reduced arousal is managed by minimizing the causative factors contributing to reduced arousal coupled with frequent sessions of mobilization and the upright position to stimulate arousal, promote greater tidal volumes and alveolar ventilation, increase zone 2 (area of optimal ventilation and perfusion matching), increase FRC, and minimize closing volume. Most often in a given patient, atelectasis results from a combination of these factors, thus necessitating a multipronged approach in its management. Breathing control and coughing maneuvers augment the cardiovascular and pulmonary physiological effects of mobilization and body positioning. Coordinating these interventions distributes ventilation more uniformly rather than directing gas to already open alveoli, which overdistends these units. The distribution of ventilation has long been known to be altered primarily by body positioning rather than deep breathing.23 Sustained maximal inspiratory efforts may augment alveolar ventilation; however, the parameters necessary for such efforts to be maximally therapeutic remain to be elucidated. If impaired mucociliary transport or excessive secretions are obstructing airways and contributing to atelectasis, mobilization of pulmonary secretions is the goal. Mobilization and a physiological stir-up regimen24 are instituted as soon as possible for multiple reasons in patients who are acutely ill to augment oxygen transport and minimize reduction in aerobic capacity (Chapter 18). In the event of excessive secretions, mobilization may need to be more vigorous to stimulate eucapnic deep breaths and inspiratory efforts and, hence, effective coughs. Stir-up, coined 70 years ago by Dripps and Waters25 aptly describes the clinical role of physiologically perturbing a patient to reduce risk and improve outcomes.
Individuals with Acute Medical Conditions
Cardiovascular Pathology
Hypertension
Pathophysiology and Medical Management
Principles of Physical Therapy Management
Angina
Pathophysiology and Medical Management
Principles of Physical Therapy Management
Cardiac Rehabilitation
Pulmonary Rehabilitation
After anginal attack, myocardial infarction, operative procedures including bypass surgery and valve surgery
After acute exacerbation or thoracic surgery (e.g., admission lung resection)
Optimize oxygen transport by directing treatment to the underlying limitations of structure and function (impairments)
Optimize oxygen transport by directing treatment to the underlying limitations of structure and function (impairments)
Risk factors assessment
Risk factor assessment
Assessment of knowledge deficits and learning style
Assessment of knowledge deficits and learning style
Readiness to change assessment
Readiness to change assessment
Predischarge submaximal exercise test
Predischarge submaximal exercise test
Discharge lifestyle recommendations:
Discharge lifestyle recommendations:
 Smoking cessation
Smoking cessation
 Smoking cessation
Smoking cessation
 Nutrition and weight control
Nutrition and weight control
 Nutrition and weight control
Nutrition and weight control
 Physical activity and exercise
Physical activity and exercise
 Physical activity and exercise
Physical activity and exercise
 Stress management
Stress management
 Stress management
Stress management
Plan for follow-up
Plan for follow-up
Uncomplicated Myocardial Infarction
Pathophysiology and Medical Management
Principles of Physical Therapy Management
Pulmonary Pathology
Atelectasis
Pathophysiology and Medical Management
Principles of Physical Therapy Management
Individuals with Acute Medical Conditions



