The impact of sugar-sweetened beverages (SSBs) on blood pressure (BP) has been debated, with some evidence suggesting that their increased intake is related to higher risk of developing hypertension. We conducted a systematic review exploring the relation between consumption of SSB and BP. A comprehensive search in 5 electronic databases along with a bibliography search was performed. The keywords “sugar sweetened beverages,” “sugary drinks,” “added sugars,” “blood pressure,” and “hypertension” were indexed in all combinations. Studies were included that reported the effects of intake of SSBs on BP. We excluded studies with <100 subjects and those involving subjects aged <12 years. Of 605 potentially relevant studies, a total of 12 studies (409,707 participants) met our inclusion criteria; 6 were cross sectional studies, whereas the rest were prospective cohort studies. All 12 studies showed positive relation between increased SSB intake and hypertension; however, statistical significance was reported in 10 of these studies. Of the 12 studies, 5 reported an increase in mean BP whereas 7 reported an increase in the incidence of high BP. In conclusion, our systematic review shows that the consumption of SSBs is associated with higher BP, leading to increased incidence of hypertension. Restriction on SSB consumption should be incorporated in the recommendations of lifestyle modifications for the treatment of hypertension. Interventions to reduce intake of SSBs should be an integral part of public health strategy to reduce the incidence of hypertension.
Sugar-sweetened beverages (SSBs) are the largest source of added sugar in our diet. They include any beverage to which a caloric sweetener has been added. In the United States, high-fructose corn syrup (HFCS) is the major source of added sweeteners in sweetened beverages. There has been a 40% increase in HFCS consumption over the last 30 years, which is higher than any other food product. In the year 2000, 42% of added sugar in food products was in the form of HFCS. On an average day, 67% of adults and 4 in 5 adolescents consume SSBs in the United States. A recent report presented at an American Heart Association meeting implicated 180,000 deaths/year to consumption of SSBs. The American Heart Association recommends consumption of no more than 450 calories/week from SSBs. SSBs and their impact on health have been extensively studied over the last 15 years. Consumption of SSBs has been shown to cause an increased risk of obesity, metabolic syndrome, type 2 diabetes mellitus, heart disease, gout, and kidney stones. Recent meta-analyses have confirmed these findings by showing that SSBs are associated with a 26% increased risk of diabetes mellitus and a 20% increased risk of metabolic syndrome. To date, no systematic review has been done to summarize the studies that examined the effects of SSBs on blood pressure (BP). The objective of our review is to summarize the studies evaluating the relation between SSBs and BP.
Methods
We searched MEDLINE, MEDLINE In-Process and Other Non-Indexed Citations, EMBASE, Allied and Complementary Medicine Database, and PsycINFO to identify all the relevant studies up to August 2013. The detailed search strategy is explained in the Appendix . The keywords “sugar sweetened beverages,” “sugary drinks,” “added sugars,” “blood pressure,” and “hypertension” were indexed in all combinations for original reports and clinical studies including cross-sectional studies, observational studies, clinical trial studies, and reviews. These reports were evaluated against an a priori inclusion and exclusion criteria. Additionally, we checked reference lists of other published reviews and relevant reports to identify any additional studies. We limited our search to “human studies” and “English language articles.” Two independent reviewers examined titles, abstracts, and full reports for eligibility. We resolved discrepancies by mutual discussion and consensus.
All the studies that measured and reported the effects of SSBs on BP or on the incidence of hypertension were included. We looked at studies involving subjects aged ≥12 years. We excluded studies that did not specifically mention the effects of SSBs on BP, studies involving children aged <12 years, and studies with <100 participants.
We extracted the details on study design and methods, sample size, beverage category, and final outcome on BP. Quality assessment of the studies was conducted by 2 independent reviewers using the Newcastle-Ottawa Scale for observational studies as a guide. The quality of the studies was further evaluated for selection, attrition, performance, detection, and reporting biases. A final quality grade from A to C was assigned to each study. We resolved discrepancies in quality rating grades by discussion and mutual consensus.
Results
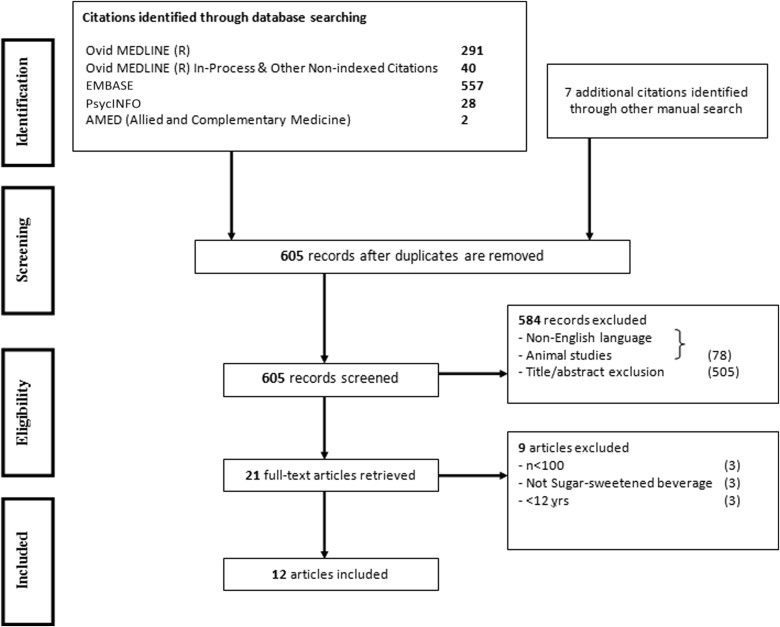
We identified a total of 918 reports in electronic databases. A manual search performed through the reference lists of relevant reviews and reports yielded 7 additional studies. Detailed schema is explained in preferred reporting items for systematic reviews and meta-analyses diagram ( Figure 1 ). After deduplication and title and abstract screening of 605 reports, we retrieved 21 potential full-text reports for in-depth evaluation. On full-text review 9 of these articles were excluded for various reasons as mentioned in Figure 1 .
The final 12 studies consisted of 6 cross-sectional and 6 prospective analyses of observational cohort studies. None of the studies showed a beneficial effect on BP from SSB consumption. In this review, 10 of the 12 studies showed a positive relation between increased SSB intake and high BP. The other 2 studies, although showing a positive trend, failed to show an association at a statistical level. These effects are illustrated in Figures 2 and 3 . Figure 2 depicts 7 studies that show that increased consumption of SSBs is associated with higher odds of increased incidence of hypertension. Figure 3 illustrates 5 studies showing an average increase in systolic blood pressure (SBP) with increased SSB consumption.
Table 1 summarizes the cross-sectional studies showing association between SSBs and hypertension. The overall relation between consumption of SSB and BP is positive. All 6 studies employed interviewer-administered recall-based structured food frequency questionnaires for dietary assessment. Three studies reported that the odds of becoming hypertensive range from 26% to 70% with increased consumption of SSBs. The other 3 studies reported increase in the mean BP. They found 0.16- to 1.6-mm Hg increase in mean SBP with increased SSB intake. Four of 6 studies involved the US population, as they were based on the National Health and Nutrition Examination Survey (NHANES). Cross-sectional analysis of these surveys showed a positive association of SSB intake with incident hypertension. Nguyen et al in 2009 and Kim et al in 2012 used NHANES data from different years (1999 to 2004 and 2003 to 2006) for different age groups, 12 to 18 years and ≥19 years, respectively, and came to similar conclusions. In a multivariate model of a relatively younger cohort, Kim et al concluded that adolescents who consumed SSBs ≥3 times/day had an 87% increased risk of becoming hypertensive. Nguyen et al reported a mean increase of 0.17 mm Hg of SBP in subjects who consumed >36 fl oz of SSBs per day. Similarly, Jalal et al in 2010 and Bremer et al in 2009 used the exact same NHANES data as previously was done by Nguyen et al and Kim et al, respectively. In addition, they added 1 extra year in their inclusion criteria. They used ≥18 years instead of ≥19 years for NHANES 1999 to 2004 and 12 to 19 years instead of 12 to 18 years for NHANES 2003 to 2006. As expected, Jalal et al concluded that consumption of 2.5 sugary soft drinks per day is independently associated with a higher risk of having increased SBP, whereas Bremer et al showed that each additional SSB serving (8 fl oz) resulted in an increase in SBP of 0.16 mm Hg (p <0.05). Later, the multicenter International Study of Macro and Micronutrients and Blood Pressure (INTERMAP) study confirmed these findings by showing that increased SSB intake of 1 serving (12 fl oz) was associated with 1.6-mm Hg increase in SBP.
| Study | Population (yr) | Sample Size | Age (yrs) | Sweetener Used | Dietary Assessment | Statistical Test/Model Used | Confounder Adjustment ∗ | Grade |
|---|---|---|---|---|---|---|---|---|
| Jalal et al | NHANES (2003–2006) | 4,528 | ≥18 | HFCS | Interviewer-administered recall-based FFQ | Univariate modeling | Yes | B |
| Tayel et al | School children in Egypt (2013) | 300 | 12–18 | Not mentioned | Interviewer-administered recall-based FFQ | Stepwise linear regression | No | C |
| Kim et al | NHANES (2003–2006) | 3,044 | ≥19 | HFCS | Interviewer-administered recall-based FFQ | Multivariate logistic regression | Yes | B |
| Nguyen et al | NHANES (1999–2004) | 4,867 | 12–18 | HFCS | Interviewer-administered recall-based FFQ | Multivariate linear regression | Yes | B |
| Bremer et al | NHANES (1999–2004) | 6,967 | 12–19 | HFCS | Interviewer-administered recall-based FFQ | Multivariate linear regression | Yes | B |
| Brown et al | INTERMAP (1996–1999) | 2,696 | 40–59 | HFCS, glucose, and sucrose | Interviewer-administered recall-based FFQ | Multiple regression analyses | Yes | B |
∗ Confounder adjustment performed for cross-sectional analysis.
Table 2 summarizes the prospective studies showing association of SSB intake and incidence of hypertension. Five of 6 cohort studies represented the US population, and 1 prospective analysis was performed in Australia. Dietary assessment was performed by way of food frequency questionnaires implemented at various times during the studies. There was an overall positive trend of having higher BP with increased intake of SSBs. Two studies reported mean BP difference and showed 1.8- and 1.9-mm Hg increases in average SBP with increased consumption of SSBs (>1 serving/day). This is in conformity with the conclusion by the INTERMAP study investigators. Three studies of 6 reported an increase in the incidence of hypertension with increased consumption of SSBs, with an odds ratio range of 1.13 to 1.6. The only conflicting data come from a study by Ambrosini et al, of a much younger cohort, which showed no difference in BP after multivariate adjustment. Moreover, Dhingra et al in their Framingham Offspring Study also showed only a marginal increase in the incidence of hypertension with >1 serving/day of a 12-fl oz SSB (odds ratio 1.18, 95% confidence interval 0.96 to 1.44). The most noteworthy positive evidence in a prospective study comes from Chen et al who, in an 18-month long, multicenter, behavioral, randomized controlled trial, showed a reduction of 1.8 mm Hg of SBP and 1.1 mm Hg of diastolic BP by reducing 0.9 servings/day (10.5 fl oz) of SSBs. Coronary Artery Risk Development in Young Adults (CARDIA) study results attribute SSBs to be responsible for a 6% increase in the risk of hypertension ; Cohen et al displayed a 6% to 20% increase in the incidence of hypertension per 12 fl oz of SSBs. Similarly, Winkelmayer et al showed 28% to 44 % increased risk of developing hypertension with increased SSB intake. The age range of these cohorts was 14 to 75 years with the length of follow-up spanning 18 months to 38 years. This suggests that positive association between increased SSB intake and hypertension is independent of age and becomes significantly greater after 18 months of increased consumption of SSBs.
| Study | Population | Sample Size | Age (yrs) | Sweetener Used | Statistical Test/Model Used | Confounder Adjustment ∗ | Grade |
|---|---|---|---|---|---|---|---|
| Chen et al | PREMIER study | 810 | 25–79 | HFCS | Mixed-effects models | Yes | B |
| Ambrosini et al | Australian offspring cohort | 1,433 | 14–17 | Not mentioned | Longitudinal (mixed-effects) models | Yes | B |
| Dhingra et al | Framingham offspring cohort | 2,803 | 42–66 | HFCS | Multiple logistic regression | Yes | B |
| Winkelmayer et al | 2 cohorts (NHS I and NHS II) | 155,594 | 25–55 | HFCS | Multivariate adjusted regression | Yes | B |
| Duffey et al | CARDIA cohort | 2,774 | 18–30 | HFCS | Multivariable-adjusted regression | Yes | B |
| Cohen et al | 3 cohorts (NHS I, NHS II, and HPFS) | 223,891 | 25–75 | HFCS | Multivariate adjusted regression | Yes | B |
Results
We identified a total of 918 reports in electronic databases. A manual search performed through the reference lists of relevant reviews and reports yielded 7 additional studies. Detailed schema is explained in preferred reporting items for systematic reviews and meta-analyses diagram ( Figure 1 ). After deduplication and title and abstract screening of 605 reports, we retrieved 21 potential full-text reports for in-depth evaluation. On full-text review 9 of these articles were excluded for various reasons as mentioned in Figure 1 .
The final 12 studies consisted of 6 cross-sectional and 6 prospective analyses of observational cohort studies. None of the studies showed a beneficial effect on BP from SSB consumption. In this review, 10 of the 12 studies showed a positive relation between increased SSB intake and high BP. The other 2 studies, although showing a positive trend, failed to show an association at a statistical level. These effects are illustrated in Figures 2 and 3 . Figure 2 depicts 7 studies that show that increased consumption of SSBs is associated with higher odds of increased incidence of hypertension. Figure 3 illustrates 5 studies showing an average increase in systolic blood pressure (SBP) with increased SSB consumption.



