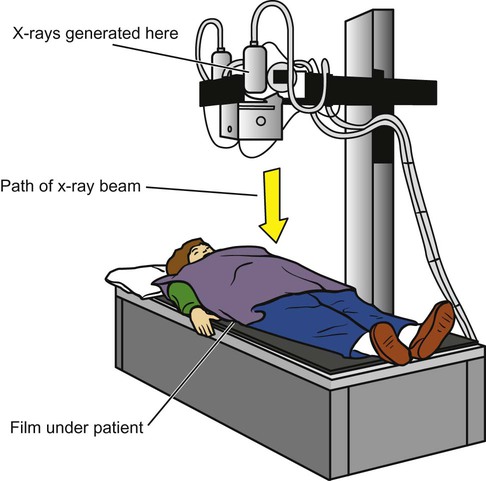
Wilhelm Roentgen discovered the x-ray in 1895 and won the very first Nobel Prize in physics (1901) for this discovery.1 Since that time, radiography has been used in medicine to image the chest structures. Ionizing radiation has its disadvantages, however, as Thomas Edison learned when his laboratory assistant, Clarence Daley, became the first scientist to die of radiation exposure in the United States.1 By the 1940s, ultrasound was being used as a way to image the body using nonionizing radiation.1 Computed tomography (CT) was developed in the 1970s, and magnetic resonance imaging (MRI) in the 1980s.1 All these methods have been used to image the chest, and each offers distinct advantages and disadvantages for the patient and the clinician. Most imaging machines still use film to capture the image, but newer systems are using digital formats. In either case, the basic methods are similar: x-rays are generated when the anode of an x-ray tube is bombarded with electrons from the cathode of the tube. The collision gives off energy in the form of x-radiation, which travels out of the tube and through the patient, then hitting the imaging cassette. The cassette contains film or a digital imaging sensor. The image is then processed by a digital processor or a film developer (Figure 11-1). The darkest images on a film (also called radiolucent areas) represent pockets of air within the body. Fat is denser than air, and it produces a dark-gray image. Muscle and other soft tissues are more dense and produce a much lighter gray image. Finally, bone is the most dense natural substance in the body and produces a white image. Metallic objects are even more dense (also called radiopaque) than bone and produce a pure white image (Figure 11-2). Figure 11-2, A, demonstrates all the different densities. This lateral view of the knee shows metal from a total knee replacement, along with bone, muscle, fat, and on either side of the patient’s knee, air.2 The x-ray image is a summation of all the densities that the x-rays have passed through. The different layers of tissue that are on top of one another are flattened into a single two-dimensional image. Sometimes the various densities lie next to one another and are easily distinguished in the image. Other times the two densities overlap one another and are blurred together in the image. For this reason, the patient is usually positioned so that two or more images can be taken at a right angle to one another. This allows structures that are overlapping in one orientation to be seen side-by-side with the other orientation.1,3
Imaging of the Chest
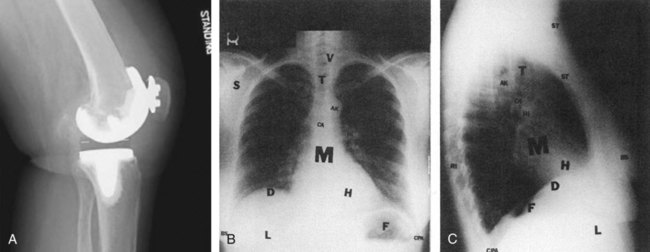
Soft tissues and extrathoracic structures: soft tissues (ST), breast shadows, (BS), diaphragm (D), liver (L), and fundus of stomach (F)
Bony thorax: ribs (RI), vertebrae (V), scapulae (S, seen best on PA), clavicles (C, seen best on PA), and sternum (S, seen best on lateral)
Mediastinal structures: mediastinum (M), trachea (T), carina (CA), aortic knob (AK), heart (H), anterior clear space (ACS, seen best on lateral), and hilus of lungs (HI)
Lung fields: hilus of lungs (HI), pulmonary vessels (arise from hilus and branch outward), costophrenic angles (CPA), and lung apices (LA, seen best on PA) (A from GE Healthcare.)
The Radiograph and Its Evaluation
Imaging of the Chest







