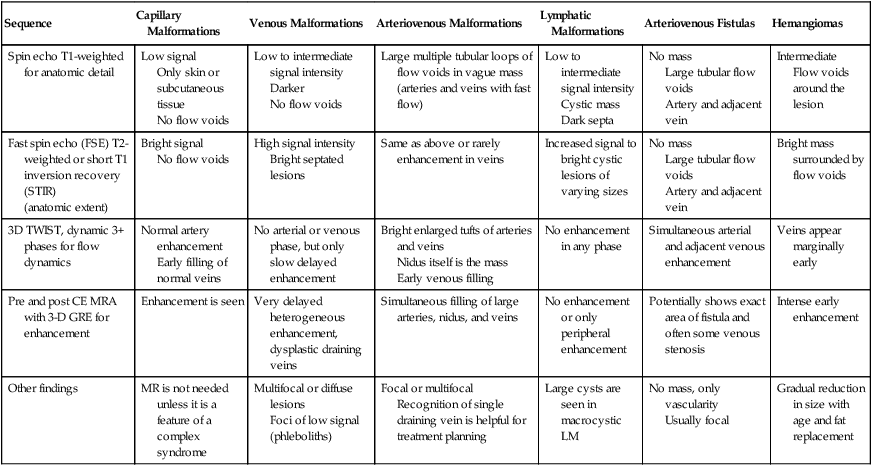
Imaging of vascular anomalies with MRI is a very complex process because it involves multiple sets of images obtained with specific protocols to enhance contrast between various tissues and also to differentiate normal from abnormal. A simplified summary of pulse sequences frequently used in evaluating vascular anomalies and findings is shown in Table 1. TABLE 1 Frequently Used Pulse Sequences and Common Findings in the Evaluation of Vascular Anomalies
Imaging of Peripheral Vascular Fistulas and Arteriovenous Malformations
Magnetic Resonance Imaging And Magnetic Resonance Angiography
Sequence
Capillary Malformations
Venous Malformations
Arteriovenous Malformations
Lymphatic Malformations
Arteriovenous Fistulas
Hemangiomas
Spin echo T1-weighted for anatomic detail
Low signal
Only skin or subcutaneous tissue
No flow voids
Low to intermediate signal intensity
Darker
No flow voids
Large multiple tubular loops of flow voids in vague mass (arteries and veins with fast flow)
Low to intermediate signal intensity
Cystic mass
Dark septa
No mass
Large tubular flow voids
Artery and adjacent vein
Intermediate
Flow voids around the lesion
Fast spin echo (FSE) T2-weighted or short T1 inversion recovery (STIR)
(anatomic extent)
Bright signal
No flow voids
High signal intensity
Bright septated lesions
Same as above or rarely enhancement in veins
Increased signal to bright cystic lesions of varying sizes
No mass
Large tubular flow voids
Artery and adjacent vein
Bright mass surrounded by flow voids
3D TWIST, dynamic 3+ phases for flow dynamics
Normal artery enhancement
Early filling of normal veins
No arterial or venous phase, but only slow delayed enhancement
Bright enlarged tufts of arteries and veins
Nidus itself is the mass
Early venous filling
No enhancement in any phase
Simultaneous arterial and adjacent venous enhancement
Veins appear marginally early
Pre and post CE MRA with 3-D GRE for enhancement
Enhancement is seen
Very delayed heterogeneous enhancement, dysplastic draining veins
Simultaneous filling of large arteries, nidus, and veins
No enhancement or only peripheral enhancement
Potentially shows exact area of fistula and often some venous stenosis
Intense early enhancement
Other findings
MR is not needed unless it is a feature of a complex syndrome
Multifocal or diffuse lesions
Foci of low signal (phleboliths)
Focal or multifocal
Recognition of single draining vein is helpful for treatment planning
Large cysts are seen in macrocystic LM
No mass, only vascularity
Usually focal
Gradual reduction in size with age and fat replacement
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


