Chapter 31 Hypoplastic Left Heart
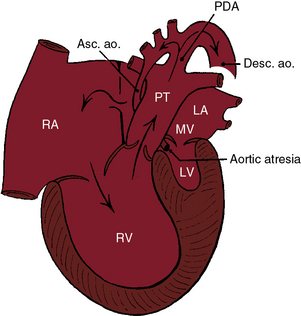
In 1952, Lev1 called attention to congenital hypoplasia of major components of the left side of the heart. In 1958, Noonan and Nadas2 referred to these malformations as the hypoplastic left heart syndrome. At the severe end of the spectrum, the aortic and mitral valves are atretic, and the left ventricle is virtually nonexistent (Figure 31-1).3,4 At the mild end of the spectrum, the aortic and mitral valves are patent, and there is a lesser degree of left ventricular hypoplasia (Figure 31-2).4 The hypoplastic left heart syndrome is a genetically heterogeneous disorder that affects 1 in 5000 live births5 and accounts for 7.5% of infants with congenital heart disease.6
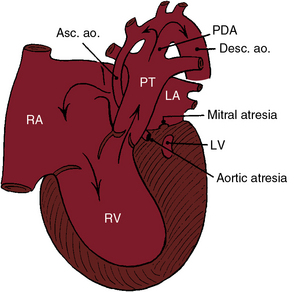
Figure 31-1 Illustration of the essential anatomic and physiologic derangements of a hypoplastic left heart with aortic atresia and mitral atresia. The left ventricular cavity (LV) is a rudimentary blind slit. The physiologic derangements are as described in Figure 31-2. (PDA = patent ductus arteriosus; ASC. ao. = ascending aorta; Desc. ao. = descending aorta.)
Aortic atresia is accompanied by a hypoplastic ascending aorta that serves as a common coronary artery (see Figures 31-1 and 31-2).7 A hypoplastic but patent mitral valve is accompanied by a hypoplastic but patent left ventricle (see Figure 31-2). Mitral atresia is accompanied by a blind slit-like left ventricular cavity embedded in the ventricular muscle (see Figure 31-1). An experimental model in chick embryos is represented by atresia or hypoplasia of the mitral valve and of the left ventricle, aortic valve, and thoracic aorta.8 Hypoplasia or atresia of the mitral valve leaves the left atrium without an exit except a restrictive patent foramen ovale (see Figures 31-1 and 31-2), which is further compromised by hypoplasia of the limbus that is rotated and deviated close to the orifice of the superior vena cava.9 An intact atrial septum is accompanied by either a thick muscular septal wall and a small left atrium or by a thick septum secundum, a thin septum primum, and an enlarged left atrium.10 Alternative decompression pathways for the obstructed left atrium consist of vascular channels from a levoatrial cardinal vein to the innominate vein, an accessory vein from left atrium to the superior vena cava, a venous connection from left atrium to hepatic veins, a coronary venous connection from left atrium to coronary sinus, and a coronary sinoseptal defect.10
Vasoconstriction during early embryogenesis leads to decreased growth and development of pulmonary veins and to alveolar capillary dysplasia, which forces arterial blood to bypass the deficient capillary bed and drain through anomalous bronchial veins.11 Lymphatics are strikingly enlarged.10 Dilated pulmonary veins are thick and arterialized with multiple elastic laminae.10
The subject of the first section of this chapter is aortic atresia with a hypoplastic but perforate mitral valve (see Figure 31-2). The second section deals with aortic atresia and mitral atresia (Figure 31-3).
Aortic atresia with hypoplastic but perforate mitral valve
The pathway to the systemic circulation is a single arterial trunk represented by pulmonary artery/ductus/descending aortic continuity (see Figure 31-2). A hypoplastic ascending aorta serves as a common coronary artery.3,12 Fifty percent to 75% of cases are accompanied by moderate coarctation of the aorta13 located either proximal to the ductus (preductal) or distal to the junction of the ductus and aortic arch (paraductal; see Figure 31-3).13 The right ventricle is hypertrophied because it is the sole pumping chamber for the systemic and pulmonary circulations.3 It harbors histologic changes of ischemia and infarction.14 The blind hypoplastic left ventricle is thick-walled and lined with endocardial fibroelastosis.2,3 Rarely, the left ventricle is characterized by isolated apical hypoplasia with fatty replacement.15 Isovolumetric contraction causes myofiber disarray but does not cause direct ventriculocoronary artery communications.16 Pinpoint neonatal aortic stenosis with small left ventricular cavity (see Chapter 7) is associated with intramyocardial sinusoids but not with direct ventriculocoronary arterial communications. The left ventricle is adequately formed in the presence of a ventricular septal defect and a patent aortic valve.3,17
The tricuspid valve is abnormal in a distinct minority of patients.18 The leaflets may be dysplastic with nodular free edges, shortened chordae tendineae, obliterated interchordal spaces, and an accessory orifice, and only two leaflets may be identifiable.18
A major concern in hypoplastic left heart syndrome is the brain that is smaller and structurally less mature than normal.19 The scimitar syndrome has been reported in a child with a hypoplastic left heart.20
The coronary circulation has been a matter of lively interest.2,3,7,14,21,22 A hypoplastic ascending aorta functions as a common coronary artery that receives retrograde systolic and diastolic flow from the patent ductus (see Figures 31-2 and 31-3).2,3,14 The tubular, hypoplastic ascending aorta is not an impediment to retrograde flow into the common coronary artery, but the preductal coarctation (see Figure 31-3) is an impediment.14 Intramyocardial coronary abnormalities analogous to those of pulmonary atresia with intact ventricular septum can be anticipated (see Chapter 24) because isovolumetric contraction generates excessive systolic pressure that acts as a driving force for direct ventriculocoronary arterial communications.7 However, the differences between pulmonary atresia with intact ventricular septum and aortic atresia with a hypoplastic but patent mitral valve are as great as the similarities.7 Myocardial sinusoids consist of restrictive vascular networks that spare the coronary arteries from the impact of high ventricular systolic pressure delivered through direct ventriculocoronary arterial communications.7 In aortic atresia with a hypoplastic but patent mitral valve (see Figure 31-2), the intramyocardial communications are sinusoidal.7 Accordingly, epicardial and subepicardial coronary arteries do not receive the impact of high isovolumetric systolic pressure and are spared the luminal obliterative features of pulmonary atresia with intact ventricular septum (see Chapter 24).7
The physiologic consequences of hypoplastic left heart with aortic atresia and a hypoplastic but perforate mitral valve are determined by the size of the ductus arteriosus, the pulmonary vascular resistance, and the condition of the atrial septum. Constriction of the ductus compromises flow into the systemic circulation and into the hypoplastic ascending aorta, which functions as a common coronary artery (see previous). Right ventricular function suffers because of the ischemic effects of inadequate coronary blood flow,14,23 because of pulmonary hypertension caused by the nonrestrictive ductus, because of high pressure in the obstructed left atrium, and because a large left ventricular mass has disadvantageous effects on right ventricular end-diastolic volume and right ventricular wall motion. Competence of the tricuspid valve is important for survival, yet tricuspid dysplasia with a multiple papillary muscles is common (see previous). Low pulmonary vascular resistance permits increased pulmonary arterial blood flow that is received by the obstructed left atrium from which the only effective egress is a restrictive patent foramen ovale (see previous; see Figure 31-2). In the presence of an adequate interatrial communication, increased pulmonary blood flow makes a large volume of oxygenated left atrial blood available for mixing in the right atrium, so systemic arterial oxygen saturation is relatively high. However, preferential blood flow into the lungs through the ductus is accompanied by a reciprocal fall in systemic blood flow and a shock-like state. When pulmonary vascular resistance is high, systemic blood flow is maintained at the price of increasing cyanosis.
History
Hypoplastic left heart comprises 7% to 8% of symptomatic heart disease in the first year of life24 and is responsible for 25% of cardiac deaths in the first week of life.6 The malformation has been called the most malignant form of congenital heart disease, a conclusion underscored by an average lifespan of only 5 to 14 days.3,6,25 Precarious survival depends on three tenuous variables: patency of the ductus arteriosus, pulmonary vascular resistance, and an adequate interatrial communication.26 Tachypnea, tachycardia, and cyanosis are present during the brief interval of ductal patency.24 Risk is greatest during the period of normal ductal closure when systemic blood flow and coronary blood flow decrease or cease altogether. A fall in pulmonary vascular resistance diverts blood from the systemic circulation into the pulmonary circulation and augments flow into the obstructed left atrium. A rise in pulmonary vascular resistance improves systemic blood flow, but at the price of hypoxemia. Ninety-five percent of afflicted infants die within the first month of life.6,27 Two extraordinary survivals include a 22-year-old woman with a large patent ductus arteriosus and an adequate-sized atrial septal defect and a 24-year-old man with a patent ductus arteriosus and a ventricular septal defect.28
There is male prevalence of 55% to 70% in aortic atresia with a hypoplastic but perforate mitral valve.2,3,29 Maternal age tends to be above average, with a mean of 31 years. First-degree relatives of probands have an increased prevalence of congenital heart disease.24 The malformation is occasionally familial30,31 and has been reported in siblings as an autosomal recessive inheritance.32 A mosaic chromosomal 22q11 deletion is associated with hypoplastic left heart,33,34 and genetic disorders include Turner’s syndrome (see subsequent), trisomy 13, trisomy 18, and trisomy 21.35–37 Concordance has been reported in a monochromic twin pregnancy.38
Reports of geographic clustering implicate environmental factors.39 Eastern Wisconsin has increased rates of hypoplastic left heart syndrome,40,41 a region in Baltimore has twice the expected frequency,42 and the island of Malta has a decreased incidence.43
Hypoxemia and hypotension are associated with hypoxic-ischemic cerebral injury and intracranial hemorrhage.44 Major and minor congenital central nervous system abnormalities include microcephaly, microencephaly, abnormal cortical mantle, agenesis of the corpus callosum, and holoprosencephaly.45 The overall frequency of extracardiac anomalies, including central nervous system abnormalities, is 12% to 37%.35
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


