Today, the incorporation of medical management and that of open and endovascular therapies for cerebrovascular disease makes the vascular specialist an integral member of the health care team treating these patients. The necessity of this involvement has been proven by the success of carotid, aortic arch branch, and vertebral artery revascularizations for the relief of symptomatic, stenotic, or ulcerated arterial lesions, aneurysms, and vascular tumors located in these vessels. The vascular and endovascular surgeon may also be consulted to evaluate patients with asymptomatic cerebrovascular disease, to provide a risk assessment as well as to help determine the appropriateness of intervention for stroke-risk reduction. Currently, evaluation and analysis of the selection and performance of carotid angioplasty and stenting (CAS) versus carotid endarterectomy (CEA) and medical management continues to alter the landscape in which extracranial cerebrovascular disease is treated.
In this chapter, common clinical presentations that suggest extracranial brachiocephalic, carotid, or vertebral artery disease are discussed. Certain principles of current care that facilitate an appropriate, smooth, and safe procedure for the patient are highlighted. Finally, the management of the most common early and late complications of carotid interventions is summarized.
I. Common clinical scenarios.
A. Symptomatic carotid disease.
Symptomatic carotid occlusive disease consists of transient ischemic attacks (TIA) and stroke, or cerebrovascular accident (CVA). The socioeconomic, health care administrative, and individual health care importance of stroke is clear. In the United States, over 700,000 cerebrovascular accidents occur annually and result in 160,000 deaths. In the United States there are roughly 4 million stroke survivors with varying degrees of disability and the yearly economic burden of stroke is around 45 million dollars. Worldwide stroke is the second leading cause of death, estimated to occur in just over 5 million people per year. Approximately two-thirds of cerebrovascular accidents are due to thromboembolic events, and extracranial atherosclerosis is the major contributor. The anatomic distribution of cerebrovascular atherosclerosis has been studied, and the breakdown by location in those with disease is as follows: carotid bifurcation 38%, intracranial 33%, arch-branch based 9%, and proximal vertebral 20%.
1. Symptom classification. Classically, a TIA is defined as acute neurologic symptoms lasting less than 24 hours that completely resolve. However, the duration usually is measured in minutes, not hours. The term reversible ischemic neurologic deficit (RIND) has been used to describe neurologic symptoms that last longer than 24 hours but then rapidly resolve. CVA is defined as neurologic symptoms lasting longer than 24 hours with evident structural infarction. The term crescendo TIA, or stuttering TIA, is used when TIAs occur more frequently (progressive over 24-48 hours), yet there remains complete reversal of neurologic symptoms in between. Stroke-in-evolution is when there is no resolution of symptoms, but rather they wax and wane indicating ongoing neuron ischemia and neural tissue at risk of infarction. These are highly unstable situations. Symptoms reflective of thromboembolic events due to disease in the carotid artery or anterior circulation include hemiparesis, hemiparesthesias, transient monocular blindness (amaurosis fugax), or difficulties with speech (aphasia).
2. Outcomes of TIA. Approximately 75-80% of patients who suffer a stroke have had no type of preceding transient neurologic symptoms. However, the corollary is that if a patient experiences a TIA, the risk of stroke is significant. Studies have delineated a 30-50% 5-year risk of stroke once TIA occurs. In fact, recent evidence suggests that a significant proportion of this risk occurs within the first several weeks after TIA with, perhaps, a 10-25% risk of CVA within 1 month of the event. Some have even suggested that 5-10% of this risk is within hours of the event. It is, thus, critical to identify and evaluate these patients. Unfortunately, TIAs are not specific for the presence of significant carotid artery stenosis or ulcerated plaques. Only about 50% of patients with TIAs will have a tight, or hemodynamically significant, carotid stenosis (<2 mm; ≥50%), occlusion, or ulcerated plaques. The remaining 50% of patients have thromboembolism from other sources such as the heart, aortic arch, intracranial vascular disease, or no clearly evident etiology. TIAs from alternate site thromboembolism or hypercoagulability also commonly lead to stroke. However, patients with no evident etiology for their TIAs and relatively normal carotid arteries on evaluation usually follow a more benign course; they seldom suffer a stroke.
TIAs may be either hemispheric or retinal in nature. In approximately 25% of patients presenting with symptomatic carotid bifurcation atheroma, visual disturbances are the presenting symptom. Amaurosis fugax (AF) is the most common of these ocular manifestations. Transient hemianopsias and other subtle visual field defects occur less frequently. Classic amaurosis is described as a “shade coming down over the eye” for a few seconds to minutes at a time and is due to embolism to the ophthalmic artery. While the natural history of AF is somewhat more benign than hemispheric TIAs it is still significant. The stroke risk once AF arises is roughly 6-8% per year, or roughly half that in those with cerebral TIAs. And, in those experiencing visual symptoms due to cerebrovascular disease, a significant group (25%) will ultimately suffer permanent visual loss.
3. Stroke recurrence. The importance of identifying those with CVA and cerebrovascular atherosclerosis, particularly within the extracranial arteries, is due to the significance of stroke recurrence. Without treatment, those with CVA will have another stroke at a rate of between 10-20% per year, thus the 5-year gross risk is somewhere between 50% and 100%. The mortality associated with this second CVA is a staggering 35%, and events beyond the second are more than 60%. Hence, the institution of therapy is imperative.
4. Unusual presentations and symptoms of cerebrovascular disease. Rarely, deterioration in visual acuity may be due to chronic ocular ischemia (COI). Severe bilateral occlusive disease leads to a supply/demand mismatch in the retina with an increase in metabolic demand. COI is the name of the constellation of signs and symptoms related to this. Findings may include eye pain, venous stasis retinopathy, central or branch retinal artery occlusions from stagnant flow, ischemic optic neuropathy, narrowed retinal arteries, retinal microaneurysms, retinal hemorrhages, iris neovasularization (rubeosis iridis) with neovascular acute angle glaucoma, iris atrophy, corneal edema, and cataracts. This syndrome only occurs in 3-4% of those with cerebrovascular disease. Without treatment permanent blindness occurs uniformly. Another rare ocular symptom that may occur is “bright light amaurosis fugax.” This occurs because of the poor retinal blood flow causing complete white out blindness when the retina is stressed, such as going outside into the sunlight. Frequently, the vascular specialist may be asked to comment on the presence of Hollenhorst plaques and retinal artery occlusions seen on fundus examination without evidence of COI. Less than 10% of these patients will have significant carotid stenosis ipsilateral to these findings.
There are a few other uncommon symptoms of cerebrovascular disease that may be attributed to significant carotid occlusive disease. One is jaw claudication with eating due to poor ECA flow to the masseter muscle. Focal seizure activity has been noted due to atheroembolism from carotid artery disease. Pre-syncope or syncope, sometimes called drop-attacks and cognitive impairments, may rarely occur secondary to poor perfusion from significant bilateral cerebrovascular disease.
B. Asymptomatic carotid disease.
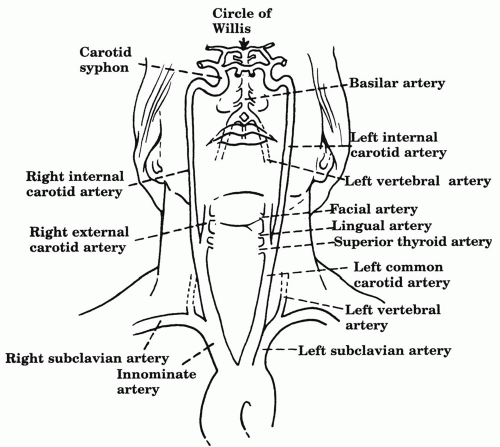
Extracranial cerebrovascular disease may also be identified in those who have no symptoms directly attributable to their arterial stenoses. Overall, only 1% of the population over the age of 65 harbors carotid occlusive disease. Yet, when focusing upon those with cardiovascular risk factors such as hypertension, hyperlipidemia, and cardiac disease this figure rises substantially to nearly 20%. This is the reasoning behind cerebrovascular screening programs, which allow recognition of those at highest risk of stroke, followed by the initiation of therapy for stroke-risk reduction. The most common initiating event for those undergoing evaluation for asymptomatic carotid stenosis is bruit on physical examination. Carotid bruits are present in approximately 5% of the general population over 50 years of age. However, only 23% of bruits are found to be associated with a hemodynamically significant stenosis (≥50%), and less than half of significant stenoses occur in the presence of a bruit. There is no correlation between the loudness of a bruit and the degree of narrowing. Thus, a bruit is neither sensitive, nor specific for significant carotid stenosis; still, with the ease of noninvasive imaging, the status of the carotid artery when a bruit is detected is relatively simple. A neck bruit may originate from the carotid arteries or be transmitted from the aortic arch or heart, such as with transmitted murmurs (Fig. 13.1).
Also, not infrequently, vascular specialists are asked to consult on patients with atypical symptoms, and noninvasive imaging is performed to establish the status of the carotid arteries. Usually, the symptoms are found to be unrelated to the carotid arteries, yet a stenosis is identified. When asymptomatic carotid stenoses are identified, some 10-15% will progress to a severe category. Therefore, the management of those with asymptomatic carotid artery stenosis has become a very germane issue.
Figure 13.1. Anatomy of the aortic arch and extracranial cervical arteries. The internal carotid artery has no branches in the neck.
II. Imaging of cerebrovascular disease.
A. Duplex ultrasound.
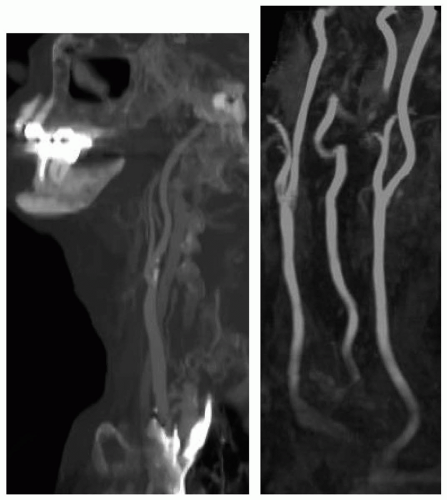
With the advent of noninvasive vascular laboratories and the establishment of duplex ultrasonography, this is the initial imaging modality of choice for most patients in which a diagnosis of carotid artery disease is entertained (see Chapter 6). Duplex ultrasound combines brightness-mode (B-mode) ultrasound with pulsed-wave Doppler to produce a real time gray-scale image of the arteries, as well as spectral analysis of flow (Figure 13.2). Many criteria have been espoused that attempt to identify and quantify the degree of carotid stenosis using duplex ultrasound. This is an ongoing process and requires regular correlation with other imaging modalities in order to solidify each noninvasive laboratory’s exactness. When performed by skilled vascular technologists, this imaging approach is quick, sensitive, specific, and highly accurate, and also carries no risk. Indirect evidence of arch-based and intracranial stenosis may be present but no direct imaging in these areas is possible. Transcranial Doppler may be performed in conjunction to further ascertain intracranial disease, but it cannot delineate lesion anatomy or true disease burden. The authors use the modified University of Washington criteria (Table 13.1). A greater understanding and study of duplex ultrasound in carotid occlusive disease, as well as its ease, has led to sensible surveillance regimens in those with cerebrovascular disease. This is now standard practice both in those found with moderate carotid stenosis and after carotid surgery (Table 13.2).
B. Computed tomography (CT/CTA) and magnetic resonance arteriography (MRI/MRA).
Anatomic definition and direct imaging of the brain, intracranial vasculature, archbranches, and aortic arch are valuable benefits of CTA and MRA (Fig. 13.2). Up to 10% of the time, arch-branch based disease is found to be present. In 2-5% of carotid bifurcation stenoses, either a tandem intracranial stenosis or intracranial aneurysm exists distal to the carotid lesion. Further, the status of the brain and recent or past CVA can be identified, which is particularly important in symptomatic cerebrovascular disease. With CTA, infarction cannot always be identified immediately as it often takes 24 to 48 hours for evidence of stroke to be present using this imaging modality. A benefit of CTA is the imaging of intracranial bleeding. Atherosclerotic calcification can limit CTA’s ability to characterize stenoses. MRA, on the other hand, using diffusion weighted technology, can illustrate and describe infarction immediately. A drawback to MRA is its notorious overrepresentation of stenoses. This is due to the fact MR technology depends on electron polar changes with magnetic field pulses. In standard magnetic resonance, blood flow is thus represented as signal dropout or a black appearance, since electrons do not stay in one place in the blood. If not timed appropriately, flow attributes may not be portrayed correctly, so this technology is highly institution and personnel dependent.
C. Arteriography.
The stroke risk associated with cerebrovascular arteriography is 1-2%. Access site and other complications can occur in up to 3%, which led to the development of other less invasive methods of imaging. Yet, there remain several situations where arteriography is helpful and finalizes cerebrovascular imaging. These include discordant or unreliable noninvasive studies, a high carotid bifurcation, no clear lesion endpoint seen, concern for either intracranial or archbased/great vessel disease, the possibility of nonatherosclerotic etiologies of disease, suspected posterior circulation disease as the symptom cause, recurrent stenosis, and the potential indication for endovascular treatment such as CAS or vertebral origin stenting.
Figure 13.2. CTA/MRA: Reconstructed CTA of the left carotid system(left). MRA of bilateral carotid bifurcations(right). CTA, computed tomography; MRA, magnetic resonance arteriography.
III. Treatment of carotid occlusive disease.
A. Medical therapy.
Risk factor modification is clearly indicated in patients with cerebrovascular disease (see Chapter 7). Many already have risk reduction therapies in place for hypertension, hyperlipidemia, and coronary artery disease at the time of diagnosis of carotid, great vessel, and vertebral artery disease due to the association with other cardiovascular processes. Statin therapy has been shown to be beneficial in carotid occlusive disease both in primary and post-procedural roles. Antiplatelet drugs such as aspirin and clopidogrel retard platelet aggregation and may prevent microemboli that cause TIAs and strokes. This has made these agents critical components of maintenance therapy after neurologic events and diagnosis of asymptomatic stenosis. Aspirin reduces the risk of continuing TIAs, stroke, and death by approximately 20%, compared to controls. In a randomized, blinded trial of clopidogrel (Plavix, Sanofi Pharmaceuticals, Inc., New York, NY, U.S.A.) versus aspirin in patients at risk of ischemic events (CAPRIE), clopidogrel (75 mg daily) reduced the relative risk for ischemic stroke, myocardial infarction and vascular death by 24%. After carotid endarterectomy, antiplatelet therapy reduces risk of stroke and to a lesser degree restenosis. It appears likely that antiplatelet therapies modestly reduce the risk of stroke in both symptomatic and asymptomatic individuals with cerebrovascular disease, and are indicated with minimal bleeding risk.
Table 13.1. Modified Washington duplex criteria
Stenosis
PSV
EDV
Spectrum
Normal
<125 cm/s
Normal with no plaque
1-15% (B)
<125 cm/s
Normal with plaque
16-49% (C)
<125 cm/s
Broadening
50-79% (D)
>125 cm/s
<140 cm/s
Broadening
80-99% (D+)
>125 cm/s
>140 cm/s
Broadening
Occluded (E)
No flow
No flow
No flow
PSV, peak systolic velocity; EDV, end diastolic velocity; cm/s, centimeters per second; CCA, common carotid artery; ICA, internal carotid artery; ECA, external carotid artery.
EDV: 80cm/s ˜ 60%; 100 cm/s ˜ 70%
ICA:CCA PSV ratio: 3.2 ˜ 60%; 4.0 ˜ 70%
Table 13.2. Standard carotid surveillance protocol
Clinical Group
Frequency of Surveillance Duplex
B lesion and C lesion
Every 1-2 years
D lesion without CEA
Every 6 months
Post CEA
Every 6 months for 2 years, then yearly or based on contralateral stenosis
Contralateral carotid occlusion
Every 6 months
Post CAS
Every 6 months
CEA, carotid endarterectomy; CAS, carotid angioplasty and stenting.
Heparin or warfarin sodium (Coumadin, DuPont Pharmaceuticals Company, Wilmington, DE, U.S.A.) can also control TIAs in at least 90% of patients with recent onset. Warfarin also has proved effective in reducing serious cerebral infarct from 45% in untreated patients to 24% in treated individuals over 5 years. Of course, the main disadvantage of long-term Coumadin therapy is compliance and bleeding complications in about 15% of patients. Indeed, the current recommendations from the multispecialty guidelines council has recommended heparin not be used in acute stroke due to the hemorrhagic risk.
B. Surgical therapy.
Perhaps nothing in vascular disease has been scrutinized more closely than CEA. During CEA the carotid artery is clamped and opened, and the atherosclerotic plaque is removed. Large, multicenter prospective, randomized trials comparing this operation plus antiplatelet therapy to antiplatelet therapy alone have provided many insights into this surgical option. In patients with a hemodynamically significant carotid stenosis, who have had a TIA or a stabilized, nondisabling stroke and are candidates for operation, CEA reduces the risk of recurrent stroke. This was clarified in both the North American Symptomatic Carotid Endarterectomy Trial (NASCET) and the European Carotid Surgery trial (ECST). The Veterans Affairs Trial 309 (VA 309) also found a trend favoring surgery, but was halted when the initial results of NASCET and ECST were reported. NASCET’s evaluation of those with high-grade (≥70%) stenosis was stopped early as the risk of stroke at 2 years was 26% versus 9% (p<0.001), and mortality 12% versus 5% (p<0.01), in the medical and surgical arms, respectively. Stroke-risk reduction increased as the degree of stenosis became greater. Thus, those with the most significant degree of stenosis gleaned the highest degree of absolute benefit. For those with carotid stenosis of 50-69%, NASCET revealed a significant reduction in ipsilateral stroke (15.7% vs. 22.2%; p = 0.045) and any stroke or death (33.3% vs. 43.3%; p = 0.005) at CEA 5 years. Although still statistically noteworthy, the absolute risk reduction was less than in those with higher-grade stenoses and was not as evident until the later points of follow-up.
In ECST and the VA 309 similar outcomes were found. Data generated from the pooling of these three trials has confirmed the stepwise augmentation in stroke-risk reduction with CEA by increasing stenosis degree. Carotid stenosis of 50% was confirmed to be the point at which CEA yields significant absolute 5-year stroke-risk reduction compared with medical therapy. Above 60-70% was the degree to which significant 3-year absolute stroke-risk reduction occurred. Benefits of CEA in the symptomatic pro spective, randomized trials appear to be greatest in men, those with recent stroke, and hemispheric symptoms.
When symptomatic patients are encountered, several questions can lead to sensible management.
1. Is there a significant carotid stenosis? The imaging modalities discussed earlier are used. Duplex ultrasound is the first-line modality, which helps to delineate degrees of carotid stenosis and important plaque characteristics such as ulceration, as well as indirectly attempting to find evidence of proximal arch-based disease and poor vertebrobasilar flow. Additionally, the anatomic location of the carotid bifurcation and the presence of an identifiable lesion endpoint with normal appearing distal internal carotid artery (ICA) are important features. The spectral analysis of flow may reveal a resistive pattern suggesting distal intracranial disease. In many patients, particularly those with TIA, carotid duplex scanning may provide enough anatomic and functional information to proceed with CEA without alternative imaging.
If any feature of the cerebrovascular circulation is not well appreciated, or there is concern for recent stroke, alternative noninvasive imaging is indicated. This may consist of an MRA or a CTA. Findings that may necessitate carotid arteriography after duplex and or CTA/MRA are as follows: discordant or unreliable noninvasive studies (i.e., the studies conflict one another), a high carotid bifurcation precluding complete duplex imaging, absence of a visible lesion distal endpoint on duplex or CTA/MRA, concern for tandem disease in the intracranial or intrathoracic carotid segments, suspicion of posterior circulation disease and/or the presence of recurrent stenosis months or years following CEA. In one or more of these instances, arteriography will finalize imaging and evaluation of the degree of stenosis and lesion morphology. Today, some of these features may lead to endovascular therapies such as CAS at the time of diagnostic arteriography.
2. Are the symptoms actually consistent with TIA or CVA, or some other neurologic or psychosomatic complaint? Are they attributable to events ipsilateral to the carotid stenosis? These questions are not always easy to answer. As noted, carotid distribution symptoms classically include unilateral hemiparsis, hemiparesthesias, speech disturbance, or amaurosis fugax. The symptoms that present confusion in determining whether a true TIA, or potential CVA, is being experienced are atypical complaints, especially dizziness, lightheadedness, presyncope, and unsteady gait. These posterior circulation type symptoms are rather common in elderly patients who may experience postural hypotension when arising quickly from a lying, sitting, or stooping position and other etiologies that produce these sensations. If a psychosomatic problem is suspected, a careful inquiry about family or work situations may disclose emotional stress that initiates the symptoms. If the patient is unsure of the symptoms, a family member who may have observed an attack can be very helpful.
3. Are the neurologic symptoms chronic and stable or repetitive and progressive, and has the patient had a stroke? If they represent TIA and are not suggestive of CVA and are not progressive, a more elective/urgent outpatient evaluation is appropriate. Remember, however, the newer, more worrying up-front risks of TIA. If the symptoms are concerning for a new or recent stroke or are progressive and repetitive, suggesting either crescendo TIA or stroke-in-evolution, immediate or urgent assessment is indicated. Thorough evaluation for TIAs may also require electrocardiographic monitoring (Holter monitor) to detect arrhythmias or echocardiography to rule out diseased heart valves or mural thrombus. Transesophageal echocardiography may also reveal ulcerative atherosclerosis of the aortic arch as a source of thromboemboli in some patients. Moreover, electroencephalography (EEG) is appropriate if a seizure disorder is suspected. Consultation with a neurologist or ophthalmologist may be helpful in evaluating patients if atypical neurologic or retinal symptoms are present. In those with atypical symptoms, or concern for stroke, computed tomography (CT/CTA) or MRI/MRA of the brain is useful to not only better clarify the extent of cerebrovascular disease, but to identify stroke and check for hemorrhage. MRI with diffusion weighting is particularly useful for this. It can identify stroke immediately while CT takes several days for the stroke to be evident.
If the patient has had a stroke, particular aspects are relevant to possible intervention and surgical therapy. First, it is important to understand how significant and debilitating the CVA has been and if there is still brain tissue at risk for infarction. In those with dense, complete deficits such as hemiplegia and/or loss of speech, it makes little sense to put the patient at risk for an operation if there is little hemispheric function left to lose. Indeed, the prospective, randomized trials studying CEA for symptomatic patients only included those with TIAs and “nondisabling” stroke. Poor outcomes due to hemorrhagic conversion in those with stroke and immediate surgical intervention were encountered before CT and MR technology were developed. Since that time, there has been much controversy with regard to radiographic features of CVA and the timing of CEA. No clear consensus has been reached with regard to the timing of CEA following hemispheric stroke. What is clear is that the larger the CVA the more likely the patient is to have a permanent deficit. If there is any evidence of parenchymal hemorrhage associated with the stroke, or it is larger than 2-3 centimeters in size, it is probably wise to wait 4 weeks before CEA. If the stroke is small without hemorrhage, an earlier operation (within 14 days) can be performed.
Fortunately, scenarios where more emergent intervention is necessary are rare. Those with crescendo TIA should be immediately hospitalized for anticoagulation with heparin (loading dose of 5,000 to 10,000 units, with a continuous hourly infusion of 750 to 1,000 units) to achieve an aPTT of 60-90 seconds or an antifactor Xa level of 0.4-0.7 IU/ml. If the patient’s condition is stable, an urgent MRA or CTA in conjunction with a duplex ultrasound usually is performed within 24 hours after admission. Arteriography is indicated if previously discussed features are present. Operative candidates with severe (>70%) carotid stenosis or shaggy, mobile, irregular ulcerative plaques undergo carotid endarterectomy when the surgical and anesthesia teams are optimized.
Management is more difficult if the neurologic symptoms are progressing, or waxing and waning, without complete resolution. These patients should be considered to have a stroke-in-evolution. Anticoagulation and emergent duplex ultrasound followed by immediate carotid surgery for severe carotid lesions and those with ominous plaque features may reduce the stroke severity and mortality in this group. However, the differentiation between a stroke-in-evolution and completed stroke is not always clear. This aggressive surgical strategy for crescendo TIA and stroke-in-evolution is related to a poor stroke and mortality rate with medical therapy alone in these patients. The reported mortality with these events is 50-80%, with up to 75% of survivors having a moderate to severe permanent neurologic deficit. Less than 5-10% will completely recover. With the institution of the treatment paradigm described, perioperative stroke and death rates of approximately 10-20% can be anticipated. While this is a considerable event rate after CEA it may be the patient’s best alternative. Also, treatment of acute ischemic stroke with intravenous thrombolytic therapy (tissue-type plasminogen activator) is approved for selected patients with no evidence of intracranial hemorrhage or other contraindications when started within 3 hours of onset of symptoms.
4. What is the patient’s operative risk? Combined 30-day mortality and stroke in NASCET and ECST was 5.6% and 7.0%, respectively. In general, stroke/death rates for CEA in symptomatic patients should be 5-6% or less in order for the operation to make stroke-risk reduction sense. If the patient is a poor surgical risk from a comorbidity standpoint, carotid angioplasty and stenting can be entertained. Antiplatelet and/or Coumadin therapy are medical alternatives that may be considered in this difficult scenario. Surgery or intervention should be reconsidered if antithrombotic/anticoagulant therapy fails to control the TIAs.
Based upon obtained imaging and surgical candidates with classic anterior circulation, carotid territory TIAs, or nondisabling stroke, we recommend CEA along with antiplatelet therapy for surgical correction of a stenotic plaque with ≥70% diameter reduction that correlates with the exhibited symptoms. In those with 50-69% diameter reduction, a more circumspect approach is used owing to the more modest risk reduction at later time points. If the patient clearly is healthy and has significant longevity, whereby they will glean the benefits that an operation can provide, CEA is undertaken. Other considerations causing us to lean toward surgical therapy include plaque morphology, such as ulceration or shaggy thrombus, contralateral ICA occlusion, and male gender, all of which may portend an increase in stroke risk for symptomatic patients. In those with less than 50% stenosis in the carotid artery, operation is not indicated except in very rare instances of ominous plaque morphology.
C. Surgical therapy in asymptomatic patients.
The rationale for prophylactic carotid endarterectomy for high-grade asymptomatic carotid stenosis began with the classic observations of Dr. Jesse Thompson of Dallas, Texas. In his nonoperated group, 26.8% eventually had TIAs, 15.2% experienced a nonfatal stroke, and 2.2% had a fatal stroke. On the other hand, 90% of operated patients remained asymptomatic. Only 4.5% of the operated patients developed TIAs and 2.3% experienced a nonfatal stroke.
Subsequently, Strandness and colleagues at the University of Washington used duplex prospectively to study the natural history of carotid arterial disease in asymptomatic patients with carotid bruits. The presence of or progression to a greater than 80% internal carotid stenosis was highly correlated with development of TIA, stroke, and asymptomatic internal carotid occlusion in 46% of patients compared to those lesions of 0% to 79% stenosis (1.5%). The majority of adverse events occurred within 6 months of the findings of an 80% to 99% stenosis.
Trials comparing surgical and medical therapy for carotid stenoses in those without symptoms have also been accomplished. The risk of stroke with both medical therapy and operation is less in patients who are asymptomatic. Overall, the Asymptomatic Carotid Atherosclerosis Study (ACAS), The Veteran’s Affairs Asymptomatic Carotid Stenosis study, and the Asymptomatic Carotid Surgery Trial (ACST), have indicated that in those with ≥60% asymptomatic stenosis, the risk of CVA at 5 years with antiplatelet therapy alone is 9-12%, or roughly 1.5-2% per year. With CEA added to antiplatelet therapy, this risk is reduced by half to 1% per year or 4-6% at 5 years. In ACAS, all in the surgical arm were required to undergo arteriography, yet some did not. In those who did, the risk of stroke with cerebral arteriography was 1.2%. The 30-day risk of stroke and death in the CEA group was 2.3% and this was estimated to be 2.7% if all had an arteriogram. Thus, arteriography accounted for about half of asymptomatic perioperative events. In the ACST, enrollment was based upon duplex ultrasound. Arteriography was not required but some did undergo arteriography prior to CEA. The 30-day stroke and death rate was 2.8% in the surgical arm and 3.1% in all CEA procedures. As with the symptomatic trials, benefit with operation was not suggested in women.
Only gold members can continue reading. Log In or Register to continue