General
Fungi are eukaryotic organisms that are found ubiquitously in the natural environment. Of the more than 1.5 million known species of fungi, the majority of infections are caused by only a small number of species. These fungi include those that are found throughout the world (e.g., Aspergillus, Candida) as well as endemic fungi that are limited to a certain geographic region (e.g., Blastomyces, Coccidioides).
For most pathogenic fungi, the lungs represent the most common site of infection, through inhalation of fungal spores from the environment.
1 Clinical presentation of fungal pneumonia can range from asymptomatic or self-limited infections of little significance to severe invasive or disseminated infections that can be rapidly fatal. The incidence of invasive fungal infections has increased considerably in recent decades, largely due to rising numbers of immunocompromised patients with acquired immunodeficiency syndrome (AIDS) or iatrogenic immunosuppression.
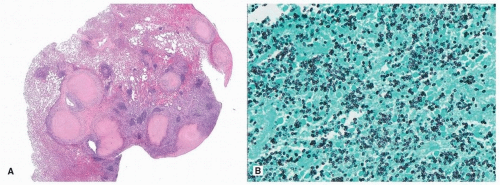
When fungal pneumonia is suspected, diagnosis thereof often requires a combination of histologic evaluation, special stains, cultures, serologic studies, and/or molecular testing. Unfortunately, tissue reactions are nonspecific and cannot be relied upon for classification of the culprit organism. These changes also vary widely depending on the patient’s immune status, ranging from robust inflammatory reactions in the immunocompetent to virtually no inflammatory response in the severely immunocompromised. In the lung, fungal infections often incite necrotizing granulomatous inflammation that forms nodules or even large cavitary masses, but poorly formed, nonnecrotizing or miliary granulomas can also be seen. Fungal infections can also produce other patterns of injury, such as diffuse alveolar damage, acute fibrinous injury, foamy alveolar casts, organizing pneumonia, acute bronchopneumonia, or airway disease. When acute lung injury is identified in a biopsy, infection should always be considered, even if organisms are not visible on the initial H&E-stained slide.
In tissue, fungi may appear as unicellular, round to oval yeasts that may display budding and/or as filamentous forms (hyphae) that may or may not be segmented (
Table 41.1). When segmentation is observed, true hyphae are distinguished by their parallel walls and discrete perpendicular septa. In contrast, pseudohyphae are formed by budding yeasts that have failed to separate, producing chains of elongated yeast forms with bulging, nonparallel walls that pinch together at the septa, akin to sausage links. These morphologic features can provide important clues to narrow the differential diagnosis, although significant overlap occurs among organisms and definitive classification is often not possible by morphologic evaluation alone.
2 Nevertheless, when fungal organisms are encountered in tissue, a pathologist should provide at least a provisional diagnosis regarding their potential identity, as well as an opinion regarding the significance thereof (invasive infection vs. allergic or saprophytic infection). This can be particularly helpful in immunocompromised patients, for whom rapid diagnosis is essential to initiate antifungal treatment, often before ancillary studies or cultures can be completed.
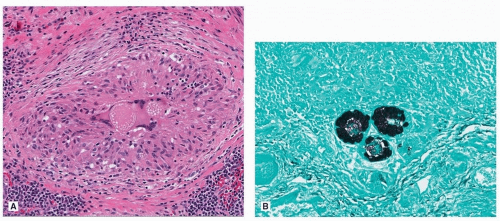
3Visualization of fungal morphology is aided by special stains, such as Gomori methenamine-silver (GMS), periodic acid-Schiff (PAS), and mucicarmine stains. Some fungi display characteristic morphologic features that can facilitate identification (e.g., the thick mucoid capsule of
Cryptococcus and the large spherules of
Coccidioides filled with endospores). However, atypical forms also occur.
4 When morphologic findings are inconclusive, ancillary studies are required. Fungal cultures, antigen detection, and serologic testing are often very helpful. Molecular PCR testing is also useful, particularly when unusual morphology is encountered.