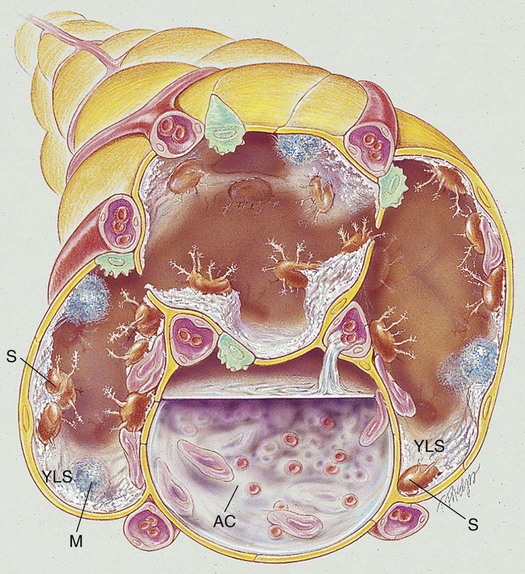
After reading this chapter, you will be able to: • List the anatomic alterations of the lungs associated with fungal disease. • Describe the causes of fungal disease. • List the cardiopulmonary clinical manifestations associated with fungal disease. • Describe the general management of fungal disease. • Describe the clinical strategies and rationales of the SOAPs presented in the case study. • Define key terms and complete self-assessment questions at the end of the chapter and on Evolve. When fungal spores are inhaled, they may reach the lungs and germinate. When this happens, the spores produce a frothy, yeastlike substance that leads to an inflammatory response. Polymorphonuclear leukocytes and macrophages move into the infected area and engulf the fungal spores. The pulmonary capillaries dilate, the interstitium fills with fluid, and the alveolar epithelium swells with edema fluid. Regional lymph node involvement commonly occurs during this period. Because of the inflammatory reaction, the alveoli in the infected area eventually become consolidated (Figure 18-1). Airway secretions may also develop at this time.
Fungal Diseases of the Lung
Anatomic Alterations of the Lungs
Fungal Diseases of the Lung