Takotsubo cardiomyopathy (TC) may be more common than previously reported in postmenopausal women (PMW) presenting with acute coronary syndrome (ACS). TC often masquerades as an ACS with electrocardiographic changes, elevated troponins, and/or chest discomfort. Its exact incidence in ACS is unknown but most studies suggest it is 1% to 2.2%. As most patients with TC are PMW, it was hypothesized that the incidence would be greater in this population. A prospective evaluation was carried out in all middle-aged and older women (≥45 years of age) presumed to be peri- or postmenopausal with an elevated troponin presenting to a community hospital over a 1-year period (July 2011 to July 2012). Troponin results above the upper limit of normal were screened on a daily basis through a computerized system. The patients’ in-hospital charts were reviewed and determined if they fulfilled the criteria for acute myocardial infarction according to the universal definition of myocardial infarction. Prespecified criteria were used to identify all patients with TC. Of the 1,297 PMW screened for positive troponins, 323 patients (24.9%) fulfilled the criteria for acute myocardial infarction and of these, 19 (5.9%) met the prespecified criteria for TC. Three additional patients with TC had acute neurologic events. Most patients (81.8%) had the apical variant. In conclusion, TC may be more common than reported in PMW with clinical and laboratory criteria suggesting acute myocardial infarction. Heightened awareness of TC in this population appears warranted.
Takotsubo cardiomyopathy (TC) is an acute condition often mimicking acute coronary syndrome (ACS) with electrocardiographic changes, elevated troponin biomarkers, and/or chest discomfort. The exact incidence of TC in ACS is still unknown but most studies suggest it as 1% to 2.2%. A recent review on this subject indicated an incidence of 2% in patients admitted for ACS and suggested that the incidence maybe underestimated. Higher rates are also predicted in specific postmenopausal women (PMW), as this group tends to be more susceptible to TC. As the above incidence includes all patients presenting with an ACS who met criteria for TC, its exact incidence in PMW is unknown. We hypothesized that as TC is more commonly seen in the elderly PMW, its incidence would be greater in this group.
Methods
The study cohort consisted of all middle-aged and older women (≥45 years of age) presumed to be peri- or postmenopausal with positive troponin-I cardiac biomarker (Siemens Centaur Assay, Siemens, Tarrytown, New York; Sensitivity >0.006 ng/ml, positive >0.04 ng/ml) who required inpatient treatment for any medical condition at a regional community hospital with Level 1 Trauma certification (Fresno, California) from July 21, 2011 to July 20, 2012. The decision to admit the patient was made by the emergency department physicians. Women below the age of 45 and men were excluded from this study. Additionally, patients who were evaluated only in the emergency department and discharged or those who died during transport or resuscitation were also excluded. One patient was included in the Takotsubo group with a typical clinical history and angiogram in whom troponins were not drawn.
Patients were further classified clinically and independent of echocardiographic and angiographic findings as those with ACS or as non-ACS according to the universal definition of myocardial infarction. Patients with acute myocardial infarction required clinical evidence and an increase and decrease of troponin.
Patient clinical variables, laboratory data, and hospital course were collected from an electronic medical record system (EPIC, version 2011, Epic Systems Corporation, Verona, Wiscosin). Echocardiographic data were analyzed in patients undergoing studies with Heart Station Software, Agfa HealthCare Corporation, Greenville, South Carolina ( http://www.agfahealthcare.com ). Echocardiographic derived ejection fraction was measured using the standard American Society of Echocardiography criteria. Angiographic studies were performed at the discretion of the attending cardiologist and digital cines were reviewed by the same interventional cardiologist to confirm the diagnosis. The diagnosis of TC was determined on basis of the review of data by independent, board certified cardiologists who were not involved in the management of the patient.
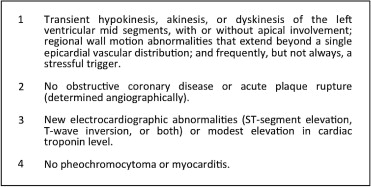
The primary outcome of the study was a diagnosis of TC. To capture all potential patients with this diagnosis, diagnostic criteria were expanded beyond the Mayo criteria to presume a diagnosis of TC. In addition to the diagnostic criteria proposed by the Mayo Clinic (see Figure 1 ), a diagnosis of TC was also suggested when those patients either met the Mayo criteria with the exception that an angiographic evaluation or follow-up echocardiography was not completed or had known coronary artery disease with typical wall motion abnormalities that were out of proportion to the diseased coronary vessel.
The incidence was calculated as a percentage of new cases during the year to the total number of patients evaluated who met the criteria for ACS. Continuous variables are displayed as mean ± 1 SD and categorical variables as percentages. Statistical calculations were performed on MedCalc statistical software (Medcalc.org, version 12.3, MedCalc Software, Ostend, Belgium).
Results
There were 1,297 patients with positive troponin-I biomarkers (Siemens Centaur Assay; positive >0.04 ng/ml). Most of these patients (75.1%; n = 974) did not meet criteria for ACS whereas the remaining 24.9% (n = 323) fulfilled an ACS diagnosis (see Figure 2 ).
Overall, there were 22 patients who fulfilled the criteria for TC (see Table 1 ). The average age of all patients with TC was 64.7 ± 11.5 years. The peak troponin was 5.9 ± 10.8 ng/ml and average ejection fraction during the episode was 34 ± 7.7%. Nineteen subjects (5.9%) who fulfilled the expanded criteria for TC met the criteria for ACS (see Figure 3 ). In patients without ACS, there were 3 cases of TC (0.3%). These 3 presented with acute neurologic conditions.
| Subject | Age | Troponin (Peak) ng/ml | ACS | Trigger | Coronary Narrowing by Angiogram | EF (%) | Season | TC Variant |
|---|---|---|---|---|---|---|---|---|
| 1 | 65 | 0.55 | + | Unknown | 0 | <20 | Summer | Apical |
| 2 | 47 | 12.60 | 0 | SAH | — | 25–30 | Summer | Apical |
| 3 | 61 | 0.80 | 0 | SAH | — | 30–35 | Summer | Apical |
| 4 | 74 | 0.08 | + | Unknown | 0 | 20–25 | Summer | Apical |
| 5 | 90 | 7.59 | + | Unknown | 0 | 35–40 | Summer | Apical |
| 6 | 82 | 35.45 | + | Assault | — | 40–45 | Summer | Apical |
| 7 | 64 | 0.51 | + | Seizures | 0 | 40–45 | Summer | Apical |
| 8 | 56 | 5.37 | + | Unknown | 0 | 30–35 | Fall | Apical |
| 9 | 64 | 0.34 | + | HCAP | — | 35–40 | Fall | Apical |
| 10 | 51 | 6.00 | + | Death of 2 sons | 0 | 40–50 | Fall | Midvariant |
| 11 | 52 | 0.37 | + | Unknown | 0 | 20–25 | Fall | Reverse TC |
| 12 | 70 | 1.10 | + | Unknown | 0 | 30–35 | Fall | Apical |
| 13 | 82 | 1.13 | + | Pyelonephritis | — | 30–35 | Fall | Apical |
| 14 | 63 | 0.28 | + | Burns | 0 | 40 | Winter | Midvariant |
| 15 | 64 | 34.55 | + | Unknown | + (1) | 35–40 | Winter | Apical |
| 16 | 54 | 0.67 | 0 | SDH | — | 35–40 | Winter | Apical |
| 17 | 66 | 5.85 | + | Unknown | 0 | 30–35 | Winter | Apical |
| 18 | 45 | ∗ | + | Unknown | 0 | 35 | Winter | Apical |
| 19 | 70 | 1.39 | + | COPD exacerbation | — | 25–30 | Spring | Apical |
| 20 | 74 | 4.95 | + | Altercation | + (1) | 25–30 | Spring | Apical |
| 21 | 70 | 1.37 | + | Sepsis | 0 | 35–40 | Summer | Apical |
| 22 | 60 | 3.68 | + | Death of cat | 0 | 40 | Summer | Midvariant |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


